
Translate this page into:
A clinical study to evaluate the efficacy of yogaraja rasayana in pandu roga (w.s.r. to iron deficiency anemia)

*Corresponding author: Manish Mishra, Department of Kaya Chikitsa, Government P. G. Ayurvedic College and Hospital, Varanasi, Uttar Pradesh, India. manish.arnav@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mishra M, Dwivedi KK, Gupta K, Kumar A. A clinical study to evaluate the efficacy of yogaraja rasayana in pandu roga (w.s.r. to iron deficiency anemia). Med India. 2024;3:64-9. doi: 10.25259/MEDINDIA_10_2024
Abstract
Objectives:
To evaluate the efficacy of Yogaraja rasayana in pandu.
Materials and Methods:
A non-randomized and open single arm study was conducted on 100 patients suffering from pandu.
Results:
The trial drug showed encouraging results in the overall health status of selected cases of pandu [with special reference (w.s.r.) iron deficiency anemia (IDA)] with >75% improvement in 61 cases and >50% improvement in 36 patients.
Conclusion:
Yogaraja rasayana is an unique herbo-mineral combination containing iron rich content ‘mandoor’ along with other herbal drugs helps in increasing the hemoglobin percentage in cases of pandu.
Keywords
Ayurveda
Pandu
Anemia
Yogaraja rasayana
Rasavaha srotodushti

INTRODUCTION
Iron deficiency anemia (IDA) is a serious global health problem involving the population of all age groups and sex. In India, IDA is most common, and the prevalence, according to the National Family Health Survey 5 (2019–21), is 25.0% in men (15–49 years) and 57.0% in women (15–49 years), 31.1% in adolescent boys, and 59.1% in adolescent girls of age 15–19 years. About 52.2% in pregnant women and 67.1% in children of 6–59 months.[1] India carries the largest burden of anemia globally, despite having an anemia control program for 50 years. Progress in reducing anemia is still slow despite substantial economic growth and 50 years of programmatic efforts. In Ayurveda, IDA can be nearly correlated to Pandu, a disease of rasavaha srotodusti.
Pandu roga is described under rasapradoshaj vikar[2] by acharya Charak, characterized as pallor on the skin, which closely resembles iron deficiency anemia (IDA) of modern science which is a reduction in the concentration of hemoglobin (Hb) in red blood cells (RBCs) that result in skin to appear pale.
Rasa and rakta are the main components of our body and function as prirnana and jeevana of shareer, respectively, as mentioned in Ashtang Hridya.[3] Rakta is considered the base of our life, which is formed in yakrut by the action of ranjaka pitta in rasa dhatu as mentioned in Susruta Samhita.[4] But when the raktadhatu gets vitiated by the doshas, mainly pitta dosha, diseases like pandu occur, which derange the rasa, bala, and sneha of the body. This, decreases the rakta and medo dhatu, thus making the body nihsaara.[5]
Dietary factors like excessive use of kshara, amla, lavana rasa, ushna, asatmaya ahara, and vegavidharana and psychological factors such as chinta, bhaya, and shoka vitiate the sadhaka pitta that resides in hridya. Vitiated vayu throws away this sadhaka pitta all over the body through dhamani, which then resides in between twaka and mamsa dhatu and results in pandutwa of skin.[6]
The word anemia is derived from the ancient Greek word anaimi, meaning lack of blood. In modern medicine, anemia refers to a decreased number of RBCs or decreased concentration of Hb in blood than normal. The normal concentration of Hb in blood ranges from 14 to 18 g/dL in males and 12 to 16 g/dL in females.
Around 30% of the total world population is anemic, and half of these have iron deficiency.
Iron deficiency occurs when iron losses or physiological requirements exceed absorption.[7] Anemia is caused by a number of factors, such as malnutrition and blood loss.
Acharya Charaka has mentioned various treatment modalities for pandu roga in Charak Samhita. Among all, Yogaraja Rasayan is considered as shrestha rasayan for pandu.[8]
Aim
The aim of this study was to evaluate the efficacy of yogaraja rasayana in pandu roga [with special reference (w.s.r.) to iron deficiency anemia (IDA)].
MATERIALS AND METHODS
Inclusion criteria
Patient with classical symptoms of pandu roga as per Ayurvedic texts.
Age between 12 and 60 years.
Patients having Hb <12% g in females and <13% g in males. Mean corpuscular volume (MCV) <80 fL, serum iron <50 ug/dL, total iron binding capacity (TIBC) >360 ug/dL, and transferrin saturation <20%.
Exclusion criteria
Patients suffering from hematological disorders such as sickle cell anemia and thalassemia.
Patients suffering from severe systemic disorders such as uncontrolled hypertension, uncontrolled diabetes mellitus, acquired immunodeficiency syndrome, and cancer.
Pregnant females and lactating mothers.
Study design
A non-randomized and open single-arm clinical study with a pre- and post- assessment was conducted in patients suffering from IDA in adolescents and elderly people.
Sample size
The sample size was 100 patients.
Sample collection
All the established cases of pandu (anemia) were registered on a specially designed Performa for the study from different out-patient departments and in-patient departments of Government P. G. Ayurvedic College and Hospital, Varanasi (U.P.), regardless of age, sex, and socioeconomic status.
Preparation of drug
The drug was prepared in the pharmacy of Government P. G. Ayurvedic College and Hospital, Varanasi (U.P.). The contents of the drug, Yogaraja Rasayana[9] are shown in Table 1.
| Content | Botanical name | Proportions |
|---|---|---|
| Haritaki | Terminalia chebula | 1 |
| Vibhitaki | Terminalia bellerica | 1 |
| Amalaki | Emblica officinalis | 1 |
| Shunthi | Zingiber officinale | 1 |
| Pippali | Piper longum | 1 |
| Maricha | Piper nigrum | 1 |
| Chitrakamoola | Plumbago zeylanica | 1 |
| Vidangamoola | Embelia ribes | 1 |
| Shilajatu | Asphaltum punjabianum | 5 |
| Rajatmakshika | Iron pyrite | 5 |
| Swarnamakshika | Chalcopyrite | 5 |
| Lauha bhasma | Iron | 5 |
| Sita | Crystallized rock sugar | 8 |
| Madhu | Honey | Adequate amount |
Method of preparation of drug
One part each of haritaki, vibhitaki, amalaki, sunthi, pippali, maricha, chitrakamoola, vidangamoola, five parts each of shilajatu, rajatmaksika, swarnamaksika, lauha bhasma, and eight-part of sita mishri (sugar) were mixed to a fine powder. This fine powder was mixed with an adequate amount of honey, made into tablet forms of 500 mg each, and was stored in a clean, airtight container.
Drug dose
The classical dose mentioned in Charak Samhita is equal to a small udumber fruit,[10] that is, 4–5 ratti (500 mg) twice a day.
Anupaan
Water.
Course of treatment
90 days.
Follow-ups
There were two follow-ups to assess the results (f1, f2) at the end of treatment.
Total duration of the entire study
One year.
Criteria for assessment
Subjective parameters
• Panduta (pallor): The score was decided on the basis of panduta present in twaka, nakha, netravartma, jihva, and hastapad tala.
| • Absent | −0 |
| • In any two of these | −1 |
| • In any three of these | −2 |
| • In any four of these | −3 |
| • In any five of these | −4 |
• Daurbalyta (weakness)
| • Not present | −0 |
| • After heavy work, relieved soon, and tolerable | −1 |
| • After moderate work, relieved later and tolerate | −2 |
| • After little work relieved later | −3 |
| • After little work relieved later but beyond tolerance | −4 |
• Hrit spandanam (palpitation)
| • Not present | −0 |
| • After heavy work, relieved soon and tolerable | −1 |
| • After moderate work, relieved later and tolerable | −2 |
| • After little work relieved later and tolerable | −3 |
| • Hrit spandanameven in resting condition and intolerable | −4 |
• Shunakshikuta shotha (periorbital edema)
| • Absent | −0 |
| • Mild | −1 |
| • Moderate | −2 |
| • Marked | −3 |
| • Severe | −4 |
• Aayasaja-shwas (dyspnea on exertion)
| • Not present | 0 | |
| • After heavy work, relieved soon and tolerate | −1 | |
| • After moderate work but relieved later | −2 | |
| • After little work but relieved later and up to tolerance | −3 | |
| • Swash even in resting condition and beyond tolerance | −4 |
• Aruchi (anorexia)
| • Normal desire for food | −0 |
| • Eating timely without much desire | −1 |
| • Desire for food, little later than normal time | −2 |
| • Desire for food only after long intervals | −3 |
| • No desire at all | −4 |
• Pindikodweshtan (cramps in calf muscle)
| • Absent | −0 |
| • Only during heavy work like exercise, climbing upstairs, lifting heavy objects, etc. | −1 |
| • During routine light works like walking, etc. | −2 |
| • Continuously throughout the day, even during resting condition | −3 |
| • Absent | −0 |
• Jwara (fever)
| • Absent | −0 |
| • Occasional | −1 |
| • Daily once | −2 |
| • Constant | −3 |
Objective criteria
Hb percentage,
RBC count,
Hematocrit value,
Mean corpuscular volume (MCV),
Mean corpuscular hemoglobin (MCH),
MCH concentration (MCHC),
Serum iron and Total iron binding capacity (TIBC).
Criteria for assessment of results
Considering the overall improvement shown by the patients in signs and symptoms, the total effect of therapy was assessed as follows: -
Complete remission - Complete relief (100%) in signs and symptoms was taken as complete remission.
Markedly improved - Patients showing improvement more than 75% in signs and symptoms were taken as markedly improved.
Moderately improved: - Patients showing improvement up to 50–75% were taken as moderately improved.
Mildly improved - Patients showing improvement up to 25–50% were taken as mildly improved.
Unchanged - Below 25% relief in signs and symptoms of pandu (anemia).
Statistically analyzed
The obtained data were analyzed statistically. The data were analyzed by Wilcoxon (Z) test.
Demographic distribution
The demographic data of registered 100 cases of pandu suggest that the maximum number of patients are observed between 25 and 55 years of age. About 65% of the total patients were female. Occupational history reveals that 78% of the total patients were housewives, socioeconomic status-wise, 91% of the total cases belonged to the middle class, and 15% of the total patients had a purely vegetarian diet.
Effect of treatment on subjective criteria
The impact of the trial drug on the classical clinical symptoms of pandu roga is shown in Graph 1. Before the treatment, panduta (pallor) showed a mean score of 2.98, which reduced to the value of 1.55 at the first follow-up (f1), indicating 47.99% relief after the first follow-up which further reduced up to the value of 0.47, indicating 84.23% relief after second follow-up (f2).
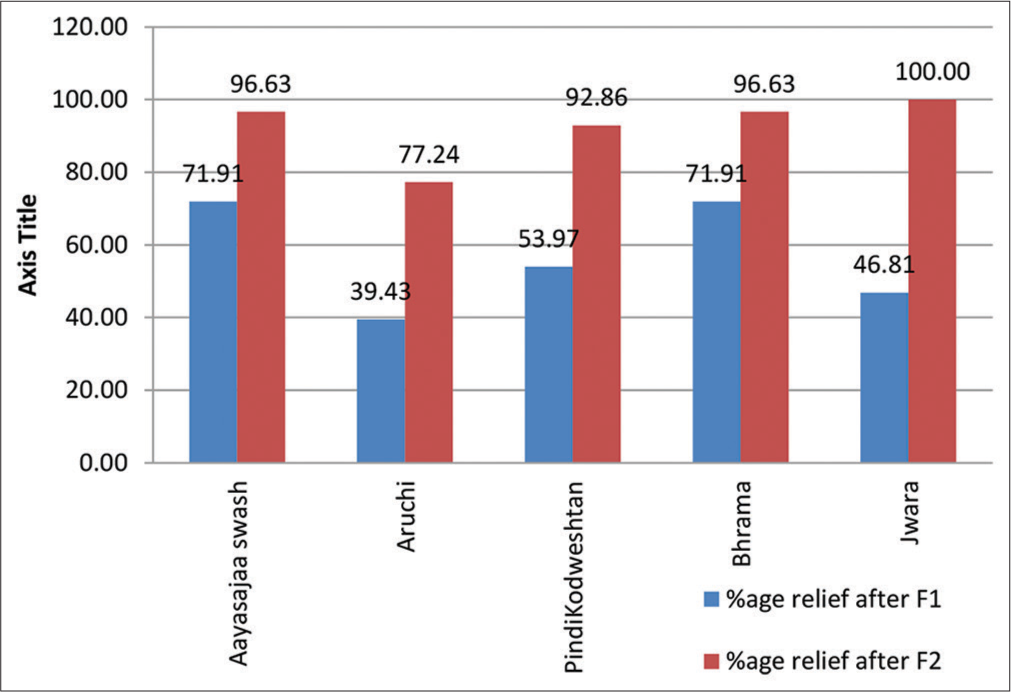
- Effect of treatment on symptoms. F1: First follow-up, F2: Second follow-up.
Daurbalyata (weakness) showed a mean score of 2.33 before treatment, which reduced to the value of 1.77 at the first follow-up (f1), indicating 49.79% relief after the first follow-up, which further reduced up to the value of 0.29, indicating 87.55% relief after second follow-up (f2).
Hridspandanam (palpitations) showed a mean score of 1.72 before treatment, which reduced to the value of 0.96 at the first follow-up (f1), indicating 44.19% relief after first follow-up, which further reduced up to the value of 0.27, indicating 84.30% relief after second follow-up (f2).
Shunakshikuta shotha (periorbital edema) showed a mean score of 2.46 before treatment, which reduced to the value of 1.49 at the first follow-up (f1), indicating 39.43% relief after the first follow-up, which further reduced up to the value of 0.56, indicating 77.24% relief after second follow-up (f2).
Aayasaja shwas (dyspnea) showed a mean score of 0.89 before treatment, which reduced to the value of 0.25 at the first follow-up (f1), indicating 71.91% relief after the first follow-up, which further reduced up to the value of 0.03, indicating 96.63% relief after second follow-up (f2).
Aruchi (anorexia) showed a mean score of 2.46 before treatment, which reduced to the value of 1.49 at the first follow-up (f1), indicating 39.43% relief after the first follow-up, which further reduced up to the value of 0.56, indicating 77.24% relief after second follow-up (f2).
Pindikodwestan (calf tenderness) showed a mean score of 1.26 before treatment, which reduced to the value of 0.58 at the first follow-up (f1), indicating 53.97% relief after first follow-up, which further reduced up to the value of 0.09, indicating 92.86% relief after second follow-up (f2).
Bhrama (delusion) showed a mean score of 0.89 before treatment, which reduced to the value of 0.25 at the first follow-up (f1), indicating 71.91% relief, which further reduced up to the value of 0.03, indicating 96.63% relief after the second follow-up (f2).
Jwara (fever) showed a mean score of 0.47 before treatment, which reduced to the value of 0.25 at the first follow-up (f1), indicating 46.81% relief after the first follow-up which further reduced up to the value of 0.00, indicating 100% relief after second follow-up (f2).
On statistical analysis, the data showed highly significant improvements in symptoms of pandu roga in both follow-ups over time (Wilcoxon-Z value: As per the table, P < 0.001) [Graph 2].
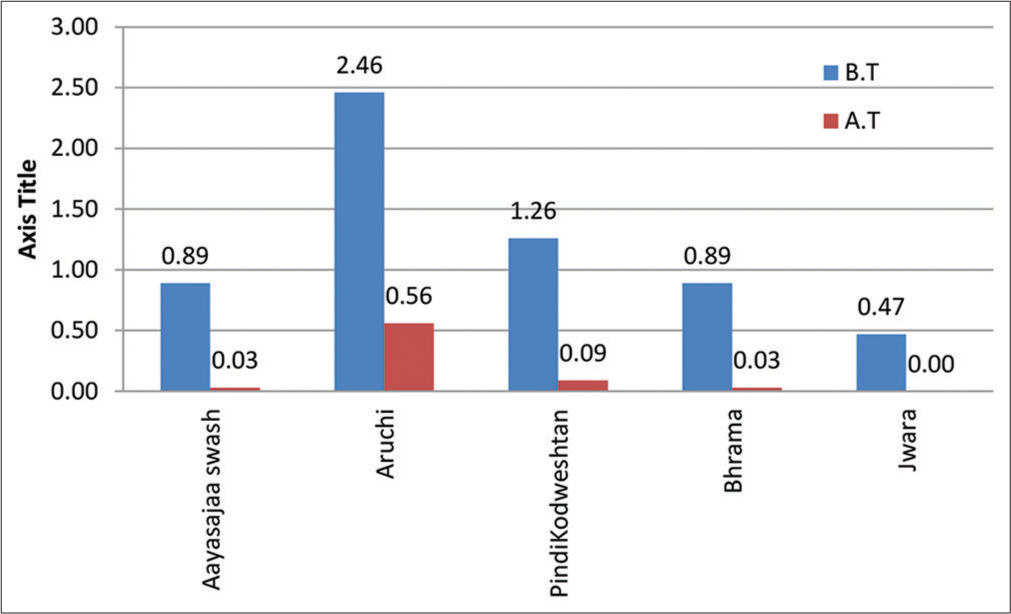
- Statistical assessment of effect on subjective criteria. B.T.: Before treatment, A.T.: After treatment.
Effect of treatment on objective criteria
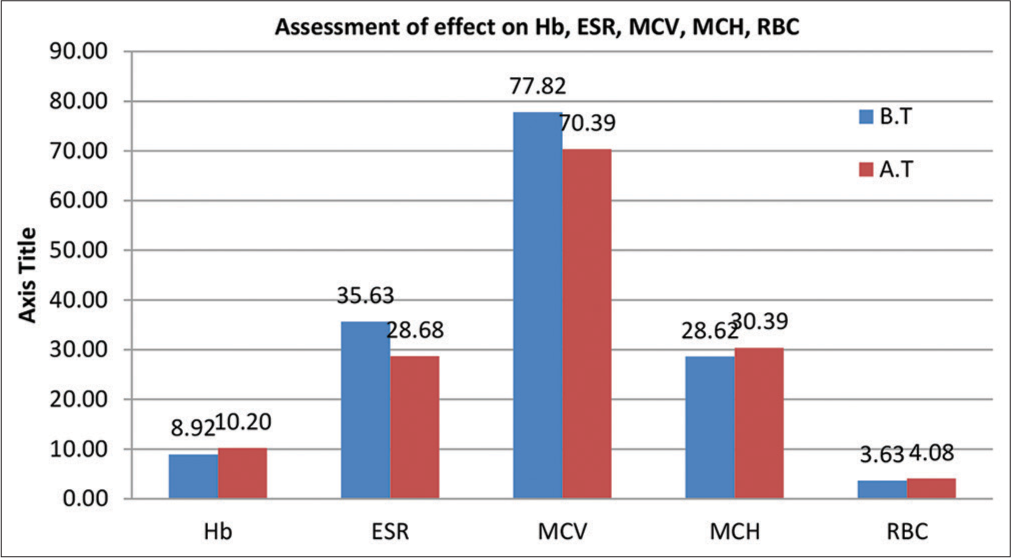
The impact of the trial drug on the objective parameters, that is, laboratory markers of iron deficiency anemia is shown in Graphs 3 and 4. Before the treatment, Hb value showed a mean score of 8.92, which increased to the value of 9.56 at the first follow-up (f1), indicating 7.22% relief after the first follow-up, which further increased up to the value of 10.20, indicating 14.31% relief after second follow-up (f2).
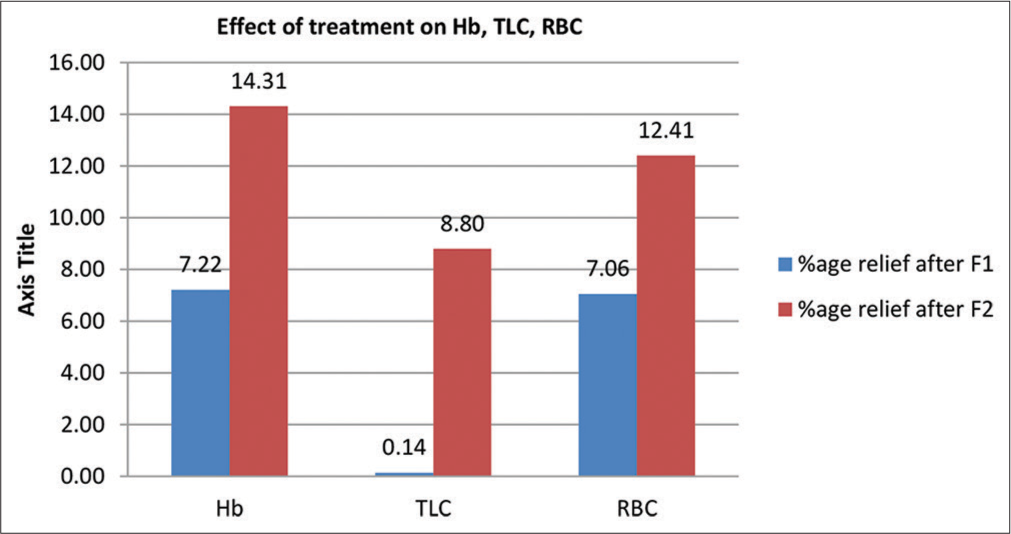
- Effect of treatment on laboratory parameters. F1: First follow-up, F2: Second follow-up.
- Effect of treatment on laboratory parameters. Hb: Hemoglobin, ESR: Erythrocyte sedimentation rate, MCV: Mean corpuscular volume, MCH: Mean corpuscular hemoglobin, RBC: Red blood cells.
TLC value showed a mean score of 1259.09 before treatment, which reduced to the value of 1257.34 at the first follow-up (f1), indicating 7.06% relief after the first follow-up, which further reduced up to the value of 1148.32, indicating 8.80% relief after second follow-up (f2).
RBC count showed a mean score of 3.63 before treatment, which increased to the value of 3.88 at the first follow-up (f1), indicating 7.06% relief after the first follow-up, which further increased up to the value of 4.08, indicating 12.41% relief after second follow-up (f2).
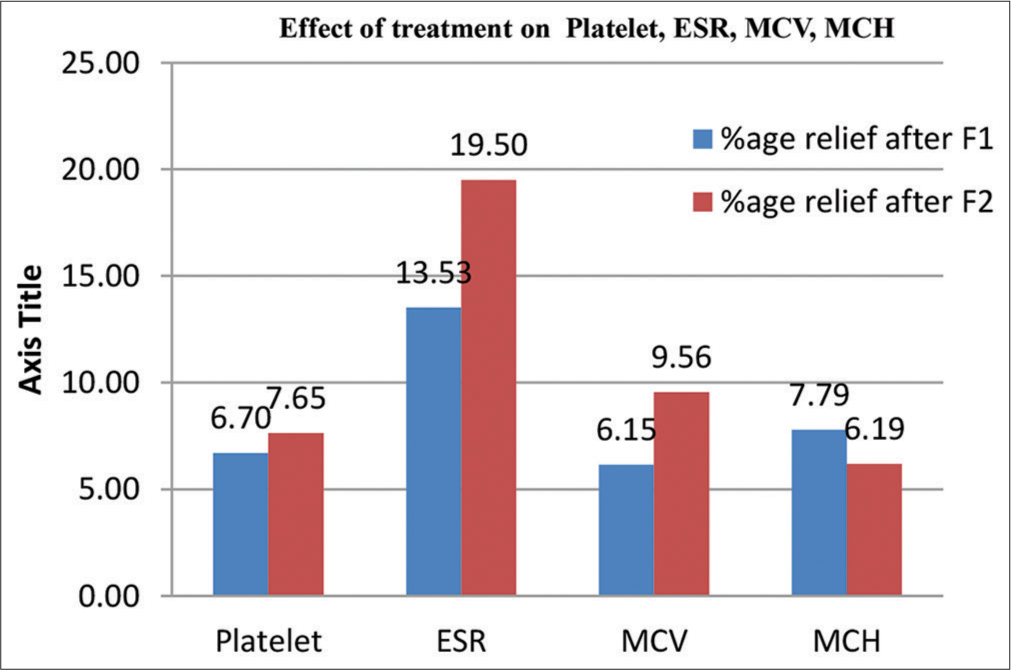
Platelet count showed a mean score of 223430.00 before treatment, which reduced to the value of 208452.00 at the first follow-up (f1), indicating 6.70% relief after the first follow-up, which further reduced up to the value of 206343.00, indicating 7.65% relief after second follow-up (f2).
ESR value showed a mean score of 35.63 before treatment, which reduced to the value of 30.81 at the first follow-up (f1), indicating 13.53% relief after the first follow-up, which further reduced up to the value of 28.68, indicating 19.50% relief after second follow-up (f2).
MCV value showed a mean score of 77.83 before treatment, which reduced to the value of 73.04 at the first follow-up (f1), indicating 6.15% relief after the first follow-up, which further reduced up to the value of 70.39, indicating 9.56% relief after second follow-up (f2).
MCH value showed a mean score of 28.62 before treatment, which reduced to the value of 30.85 at the first follow-up (f1), indicating 7.79% relief after the first follow-up, which further reduced up to the value of 30.39, indicating 6.19% relief after second follow-up (f2). MCHC value showed a mean score of 32.1293 before treatment, which slightly increased to the value of 32.3130 at the first follow-up (f1), indicating 9.64% relief after the first follow-up, which further increased slightly up to the value of 32.7440, indicating 1.91% relief after second follow-up (f2).
PCV value showed a mean score of 30.7568 before treatment, which slightly increased to the value of 33.7220 at the first follow-up (f1), indicating 9.64% relief after the first follow-up, which reduced up to the value of 33.5680, indicating 9.14% relief after second follow-up (f2).
On statistical analysis, the data showed highly significant improvements in objective parameters (laboratory markers of iron deficiency anemia) in both follow-ups over the time (Wilcoxon-Z value: As per the table, P < 0.001) [Graph 5].
- Statistical assessment on laboratory parameters. Hb: Hemoglobin, ESR: Erythrocyte sedimentation rate, MCV: Mean corpuscular volume, MCH: Mean corpuscular hemoglobin, RBC: Red blood cells.
RESULTS
After a minute assessment of observation and results and all statistical analysis, the overall treatment outcomes were assessed for 100 patients with participants categorized into three groups based on their responses: Arogya (>75% relieved), Kinchit Arogya (<75% to 40% relieved), and Anarogya, that is,<40% relief [Graph 6].
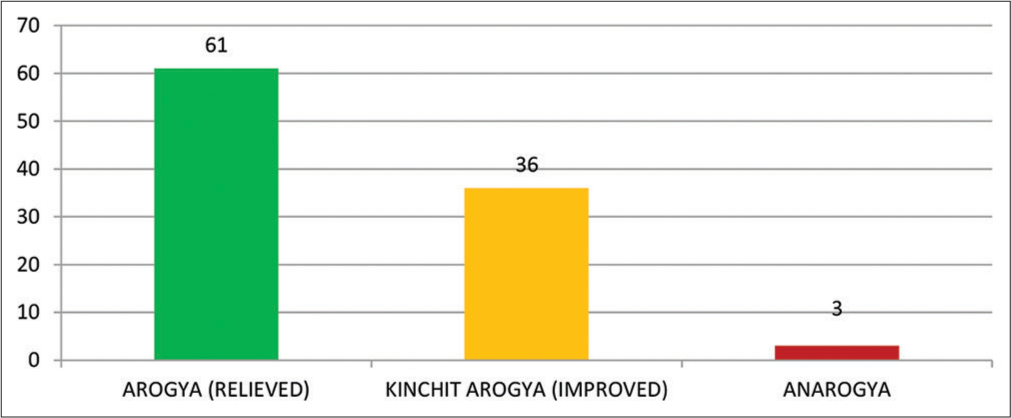
- Overall effect of the treatment.
DISCUSSION
Anemia is a serious global public health problem and is especially prevalent in women and children. Anemia in children significantly affects growth, and physical and mental development. The effects can lead to long-lasting impairment of the immune system and cognitive development. Even mild anemia can lead to fatigue and interfere with a child’s ability to perform at school.
Anemia doubles the risk of death during pregnancy and leads to poor motor and mental growth in children. Iron-deficiency anemia was also the top cause of disability in India for 10 years to 2015, India Spend reported in October 2016. Govt. of India has been running a program to overcome the condition under the name “Anaemia Mukt Bharat” since 2018.
Ayurveda says that pandu roga is a disease which occurs in the body due to doshik disturbances, that is, vitiated pitta dosha and this situation occurs due to erroneous dietary habits and lifestyle. Hence, Ayurveda focuses on complete guidance of nidan parivarjanam (refrain from pitta prakopak ahar vihar such as katu-ushna, i.e., spicy and hot food items, krodha, excessive sun bath, etc.) and pathya – apathya along with the use of aushadhi (medicine). That is the reason Ayurvedic approach has the ability to cure the disease completely.
CONCLUSION
In Ayurveda, tridosha imbalance is considered the basic and main cause of disease development. In the case of pandu roga, sadhak pitta gets vitiated. Dietary deficits and lifestyle negligence play a key role in developing pandu roga (IDA). In the modern concept, only biochemical and hematological parameters are considered mainly to diagnose the disease, and therefore, the prime source of treatment is supplementation only to correct the hematological and biochemical indices, but Ayurveda gives main consideration to pathogenesis of the disease (samprapti), so the prime source of treatment is to break the pathogenesis (samprapti-vighatan) along with replenishment of micronutrients deficit.
In our clinical study, the formulation which is used is a unique herbo-mineral combination which corrects the tridosha imbalance along with fulfilling the iron deficiency due to its iron rich content ‘mandoor.’ In this study of 100 patients of pandu, highly significant improvement was found after using ‘Yogaraj rasayana’ for three months. Hence, it can be concluded that the formulation ‘Yogaraj rasayana’ can be used as a standard control drug to treat pandu roga.
Author contributions
Dr. Manish Mishra: Guarantor, study design, data collection, principal investigator, and draft article. Dr. K. K. Dwivedi: Guarantor, conception, study design, data analysis and interpretation, and draft article. Prof. Kanchan Gupta: Conception, critical review, and final approval. Amit Kumar: Data collection and draft article.
Ethical approval
The research/study was approved by the Institutional Review Board at Government Ayurveda College and Hospital, Varanasi, U.P., INDIA, number RAC-IEC-19-I.C.Project.-01, dated January 25, 2021.
Declaration of patient consent
An informed consent was taken prior to the study on a Research Proforma especially designed for the study.
Conflicts of interest
Dr. Manish Mishra is on the editorial board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that they have not used artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript or image creations.
Financial support and sponsorship
This research is funded in part by grants from the Department of AYUSH, Government of Uttar Pradesh, under the innovation scheme for research.
References
- Anaemia Mukt Bharat. Available from: https://pib.gov.in/pressreleasepage.aspx?prid=1795421#:~:text=ministry%20of%20health%20and%20family%20welfare,anaemia%20mukt%20bharat,-posted%20on%3a%2004 [Last accessed on 2024 Jun 05]
- [Google Scholar]
- Charak Samhita, sutrasthana. Vol 1. Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 18, Verse 9-10
- [Google Scholar]
- Ashtang Sangraha, sutrasthana. Vol 1. Varanasi: Chaukhamba Prakashan; 2016. Ch. 11. Verse 4
- [Google Scholar]
- Susruta sutrasthana. Vol 1. Varanasi: Chaukhamba Prakashan; 2018. Ch. 14. Verse 4-5
- [Google Scholar]
- Charak Samhita, chikitsasthana. Vol 2. Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 16. Verse 4-6
- [Google Scholar]
- Charak Samhita, chikitsasthana. Vol 2. Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 16. Verse 8-10
- [Google Scholar]
- Blood diseases In: Davidson’s principles and practice of medicine (23rd ed). New York: Elsevier. Inc.; 2018.
- [Google Scholar]
- Charak Samhita, chikitsasthana. Vol 2. Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 16. Verse 85
- [Google Scholar]
- Charak Samhita, chikitsasthana Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 16. Verse 80-2
- [Google Scholar]
- Charak Samhita, chikitsasthana. Vol 2. Varanasi: Chaukhamba Bharti Academy; 2018. Ch. 16. Verse 83
- [Google Scholar]




