
Translate this page into:
A rare case of recurrent biballism


*Corresponding author: Ankur Banik, Department of Neurology, Medical College and Hospital, Kolkata, West Bengal, India. banik.ankur@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Banik A, Pal M, Pal S, Dutta I, Chattopadhyay A. A rare case of recurrent biballism. Med India. 2024;3:37-40. doi: 10.25259/MEDINDIA_28_2023
Abstract
Diabetic striatopathy (DS) is a relatively new entity with growing literature expanding our knowledge of the same. It is commonly seen in elderly Asian females with long-term uncontrolled type 2 diabetes mellitus presenting with hemichorea or hemiballism with characteristic reversible imaging findings involving various basal ganglia structures. While various different types of presentations with variable responses to therapy in terms of treatment modality and recovery time have been reported, there is very little data on the recurrence of this entity. We, hereby, present an interesting case of DS, which had a rare presentation in the form of biballism. Our patient had an initial swift recovery with glycemic control alone and thereafter a ropinirole-induced recurrence in spite of good glycemic control, which was rather difficult to control. This case emphasizes the need for clinicians to be aware of the various presentations of DS and to be cautious in the use of drugs with the potential to cause movement disorders in such a patient.
Keywords
Biballism
Recurrent movement disorder
Acute movement disorder
Diabetic striatopathy
Recurrent ballism

INTRODUCTION
Ballism, or ballismus, from the Greek word for “to throw,” refers to flinging or flailing movements that are non-patterned, usually involving proximal muscles of the limbs. Ballism is usually confined to one side of the body, called hemiballism; rarely, both sides are affected, called biballism. Diabetic striatopathy (DS) is a relatively new entity, and most cases present with hemichorea or hemiballism. Bilateral presentation is rather uncommon, and, biballism even more so. Nevertheless, we describe here an unusual case of biballism as a manifestation of DS, which initially completely disappeared swiftly after correction of hyperglycemia alone, but was followed by a probable drug-induced recurrence, which was far more difficult to control.
CASE REPORT
A 50-year-old male patient with long-term, poorly controlled type 2 diabetes presented with acute onset Biballism without any other neurological or systemic symptoms or signs. At that time, his initial blood glucose and hemoglobin A1c (HbA1c) were 300 mg/dL and 10.4, respectively, and his movements were promptly controlled with glycemic control alone with insulin in 3-4 days. He was discharged in stable condition with advice to continue insulin, and he was doing perfectly well. Two months later, he again developed biballistic movements of similar phenomenology and got readmitted. Seven days before the current admission, he consulted a local doctor, where he was prescribed ropinirole for suspected restless legs syndrome, and he had developed these movements 4-5 days after starting the new medication. Clinical examination was noncontributory except the biballism. Interestingly, blood glucose on admission this time around was 86 mg/dL, and regular blood glucose charting also showed normal readings throughout.
Investigations were as follows:
Complete blood count: All within normal limits (WNL)
HbA1c: 10.1
Liver, kidney, and thyroid function tests: All WNL
Serum sodium 134 mEq/L, potassium 4.2 mEq/L, and calcium 9.2 mEq/L
Viral serology (hepatitis B, C and human immunodeficiency virus HIV): All negative
Anti-nuclear antibody and autoantibody panel: Negative
Urine ketones: Negative
Serum and urine osmolality: WNL.
Imaging done during the initial and subsequent presentations is shown in the figures below. During the first presentation, the computed tomography (CT) brain revealed hyperdensities in the bilateral caudate and putamen which had almost disappeared during the subsequent event [Figures 1 and 2].
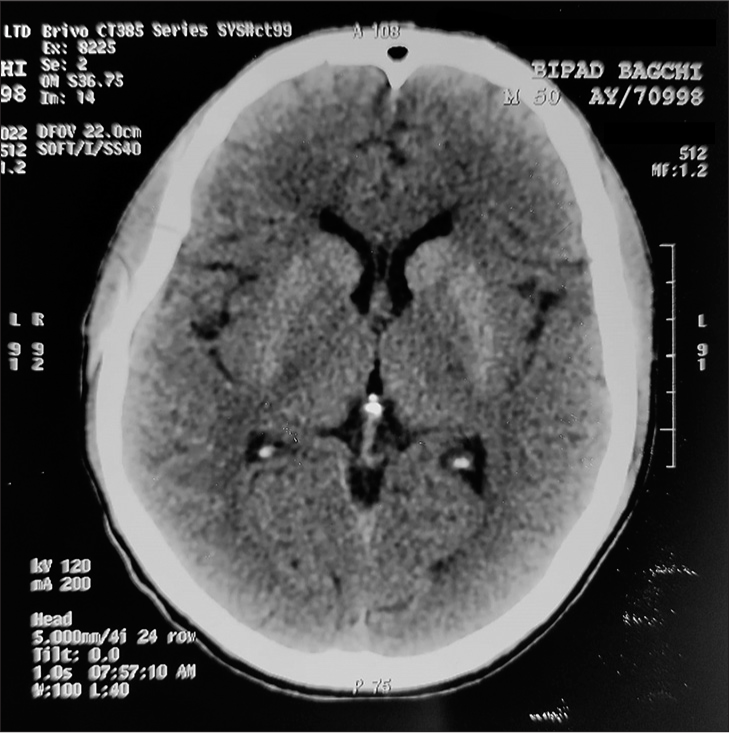
- Computed tomography brain during the initial event showing bilateral caudate and putamen hyperdensities.

- Computed tomography brain during the recurrence showing near-complete resolution of the previous findings.
This time around, although the blood glucose was well controlled throughout, and also, there was a resolution of imaging findings on CT brain; yet, his movement disorder was rather difficult to control. The newly added drugs were withheld immediately without improvement. Sequential addition of tetrabenazine, clonazepam, and risperidone was required, with which his movements gradually improved finally over a total duration of 6 weeks.
DISCUSSION
The prevalence of DS has been reported to be 1 in 100,000,[1] which is believed to be underestimated because most primary care physicians initially attending the patient might not be familiar with the condition, especially in developing countries, where it is probably more common.[2]
Bedwell, in 1960,[3] first reported a case of hemiballism in a patient with severe hyperglycemia who was treated with blood glucose-correcting drugs. Initially, hyperglycemia, as a cause of hemiballism, was reported sporadically, but now, it is considered the second most commonly reported cause after several recent reports from East Asia have provided a much more complete description of this disorder in more than 60 reported cases.[4-6] The disorder has been documented to occur predominantly in elderly females with poorly controlled type 2 diabetes mellitus. Regarding clinical presentations, the large majority of patients presented with chorea or hemichorea. Bilateral involvement was noted in only 9.7% of patients.[7] Boughammoura-Bouatay et al. have previously reported a case of biballism due to non-ketotic hyperglycemia.[8]
In patients with DS, the average levels of blood glucose and glycated hemoglobin were 414 mg/dL and 13.1%, respectively, in one study,[7] while another study mentioned an even higher HbA1c average at 14.4%.[4] In our case, the initial blood glucose was 300 mg/dL and HbA1c was 10.1, suggesting DS can occur in the background of relatively lesser grades of hyperglycemia as well than commonly reported in the literature. Of the patients undergoing an analysis of ketone bodies, the majority (81.7%) were negative for ketone bodies in their blood or urine specimens, as was the case in our patient, and various pathophysiologic mechanisms have been proposed for the same. Although traditionally subthalamic nucleus (STN) has been implicated as the site of lesions for ballism, a review of the more recent literature suggests that lesions outside of the STN accounted for as high as more than half of the reported cases.[9] The striatum is reported to be the most common non-STN site.
Although initial sporadic case studies proposed that correction of hyperglycemia usually resulted in complete or partial resolution of chorea as well as striatal abnormalities on neuroimaging studies, further subsequent studies have clearly documented that additional anti-chorea drugs might be needed in patients unresponsive to strict glucose control.[10]
In one study, 26.7% of patients received only glucose control and 73.3% received glucose control with the addition of anti-chorea medications.[7] Of the patients with documented successful treatment, the median recovery time was significantly shorter in patients undergoing glucose-control-only treatment (2 days) than in those receiving additional anti-chorea medications (14 days).[7] This was reflected in our case as well.
Since DS is itself rather new, there is very little data regarding the recurrence of the same. The recurrence rate has been postulated to be 18.2% and 13.2% in studies, and hyperglycemia has been implicated as the major cause in the few literature that is available.[7,4] In our case, since stringent blood glucose monitoring during the second episode showed persistent normal readings, hyperglycemia was unlikely to be the cause of recurrence. Ropinirole, being a dopamine agonist and being definitely temporarily related to the onset, was probably the most likely cause of the recurrence. Even then, the episode did not subside on stopping the probable offending drug and required multiple anti-dopaminergic drugs, suggesting that probably drug-induced recurrent movement disorder in the background of DS is comparatively more difficult to control.
CONCLUSION
DS can present with multiple different forms of movement disorders, including biballism, as in our case. It is far more common in non-ketotic hyperglycemia than in ketotic hyperglycemia and can manifest in a wide range of initial blood glucose and HbA1c values. Therapeutic response varies greatly, and it can even recur in about 13%-18% of cases. Although hyperglycemia is probably the most common cause for recurrence, additional probable causes for recurrence should always be sought, especially if the blood glucose levels are found to be normal. Drug-induced recurrence of movement disorder in the background of DS is probably more difficult to treat even with good glycemic control, and hence, in such a clinical scenario, drugs should be used judiciously and with utmost caution.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Hyperglycemic nonketotic states and other metabolic imbalances. Handb Clin Neurol. 2011;100:287-91.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperglycemic chorea/ballism ascertained over 15 years at a referral medical center. Parkinsonism Relat Disord. 2018;48:97-100.
- [CrossRef] [PubMed] [Google Scholar]
- Chorea associated with nonketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: A meta-analysis of 53 cases including four present cases. J Neurol Sci. 2002;200:57-62.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological and pathological changes in hemiballism-hemichorea with striatal hyperintensity. J Magn Reson Imaging. 2006;23:564-8.
- [CrossRef] [PubMed] [Google Scholar]
- Hemichorea/Hemiballism associated with hyperglycemia: Report of 20 cases. Tremor Other Hyperkinet Mov (N Y). 2016;6:402.
- [CrossRef] [PubMed] [Google Scholar]
- "Diabetic striatopathy": Clinical presentations, controversy, pathogenesis, treatments, and outcomes. Sci Rep. 2020;10:1594.
- [CrossRef] [PubMed] [Google Scholar]
- Biballism due to non-ketotic hyperglycaemia. Diabetes Metab. 2008;34:617-9.
- [CrossRef] [PubMed] [Google Scholar]
- Hemiballism: Revisiting a classic disorder. Lancet Neurol. 2003;2:661-8.
- [CrossRef] [PubMed] [Google Scholar]
- "Diabetic striatopathy" and ketoacidosis: Report of two cases and review of literature. Diabetes Res Clin Pract. 2017;128:1-5.
- [CrossRef] [PubMed] [Google Scholar]




