
Translate this page into:
Multivalvular prolapse: A case report of concurrent mitral, aortic, and tricuspid valve involvement in the same patient with severe regurgitation and heart failure features

*Corresponding author: Sai Durga Prakash, Department of Cardiology, National Institute of Medical Science, Jaipur, Rajasthan, India. prakash.d0303@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gaurab V, Bhattacharjee M, Prakash SD. Multivalvular prolapse: A case report of concurrent mitral, aortic, and tricuspid valve involvement in the same patient with severe regurgitation and heart failure features. Med India. 2024;3:86-9. doi: 10.25259/MEDINDIA_12_2024
Abstract
Myxomatous valvular disease of cardiac valves has been reported in various studies and case reports which involves mainly mitral valve. This valvular involvement produces several degrees of regurgitant lesions, causing symptoms. Concomitant involvement of mitral, aortic, and tricuspid valves has been rarely reported. Here, we report a case of a 49-year-old male with triple valve prolapse, presenting with dyspnea and palpitations. The patient was managed conservatively as he was not fit for surgical intervention. This report adds to the limited data available in the literature and current guidelines to support clinical decision-making.
Keywords
Valve prolapse
Triple valve prolapse
Myxomatous degeneration of the cardiac valves
Mitral valve prolapse
Aortic valve prolapse

INTRODUCTION
Myxomatous degeneration of the cardiac valves (MDMV) is a progressive, non-inflammatory disorder characterized by structural disarray due to a defect in mechanical integrity caused by altered synthesis and remodeling of the valve tissue, particularly involving type VI collagen.[1] While commonly associated with mitral valve prolapse (MVP), MDMV can affect other valves, although less frequently studied. We present a unique case of MDMV involving the mitral, aortic, and tricuspid valves, resulting in significant regurgitation and features of heart failure.
MDMV is most often linked with MVP, known more technically as ‘Myxomatous degeneration of the mitral valve.’ However, it can also affect the aortic and tricuspid valves, with the mitral valve being the most commonly involved (over 60%), followed by the aortic and tricuspid valves.[2] Despite the higher prevalence of MVP, there is limited literature on aortic and tricuspid valve involvement.[3,4]
The term ‘floppy valve syndrome,’ introduced by Read et al., describes valvar myxomatous degeneration, emphasizing the laxity and redundancy of the affected valves.[5] Echocardiography plays a crucial role in diagnosing this condition, with reported cases demonstrating prolapse of the aortic, mitral, and tricuspid valves, termed ‘multiple floppy valves.’[6,7]
Although myxomatous degeneration predominantly affects the mitral valve, our case underscores the involvement of multiple valves, presenting challenges in managing regurgitation and heart failure. Understanding the pathophysiology and hemodynamic consequences of multiple valve prolapse is essential for developing appropriate management strategies. By presenting this unique case, we aim to contribute to the limited literature on this topic and discuss its implications for clinical practice.
CASE REPORT
A 49-year-old male presented with complaints of dyspnea on exertion for 4–5 years. The patient was a chronic smoker for 10 years. The patient had visited a nearby hospital and was treated as a case of chronic obstructive pulmonary disease (COPD) based on X-ray findings of multiple bullae [Figure 1]. However, despite all the medication and abstinence from smoking, his dyspnea did not improve and gradually progressed. The patient also had complained of chest pain for the past three months, which was diffuse and associated with exertional exacerbation. The patient had a history of on and off palpitations. Hence, in view of the suspected cardiac cause, the patient was referred to our cardiology department for evaluation.
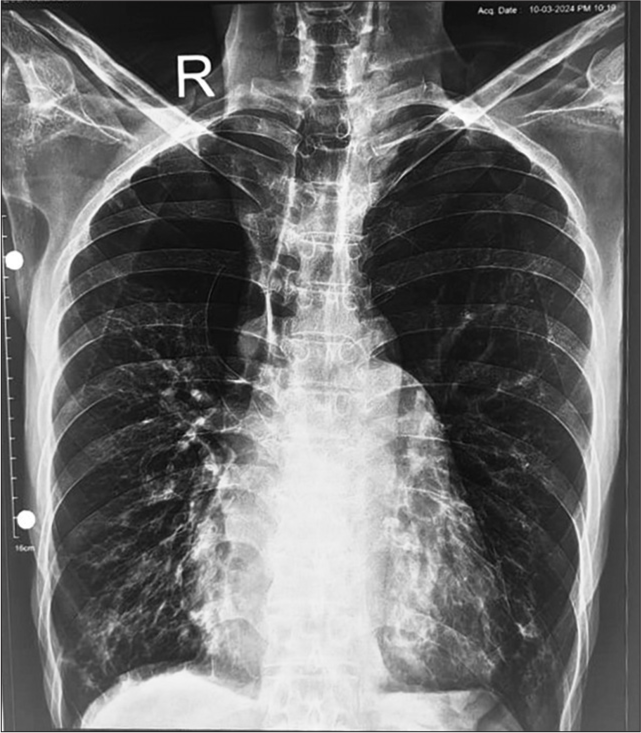
- Chest X-ray showing multiple bullae in the bilateral upper lobe.
On examination, the patient was conscious and oriented with an asthenic built. On auscultation, the patient had a systolic click with a pansystolic murmur radiating to the axilla. However, there were no features of joint hypermobility or lax joints. Even there were no features of facial or body dysmorphism. The thumb sign and wrist sign were negative. An electrocardiogram was done which showed normal sinus rhythm. Chest X-ray showed multiple large bullae in upper lung fields [Figure 1]. 2D echocardiography revealed MVP with severe mitral regurgitation (MR) and tricuspid valve prolapse (TVP) with moderate-to-severe tricuspid regurgitation (TR) [Figures 2 and 3]. For validating our findings, transesophageal echocardiography (TEE) was planned which confirmed our transthoracic echocardiogram (TTE) findings and showed aortic valve prolapse with mild AR [Figures 4 and 5]. After stabilization case was discussed with the cardiothoracic and vascular surgery team but was found to be unfit for valve replacement surgery at present. He was medically managed and advised for regular follow-up.
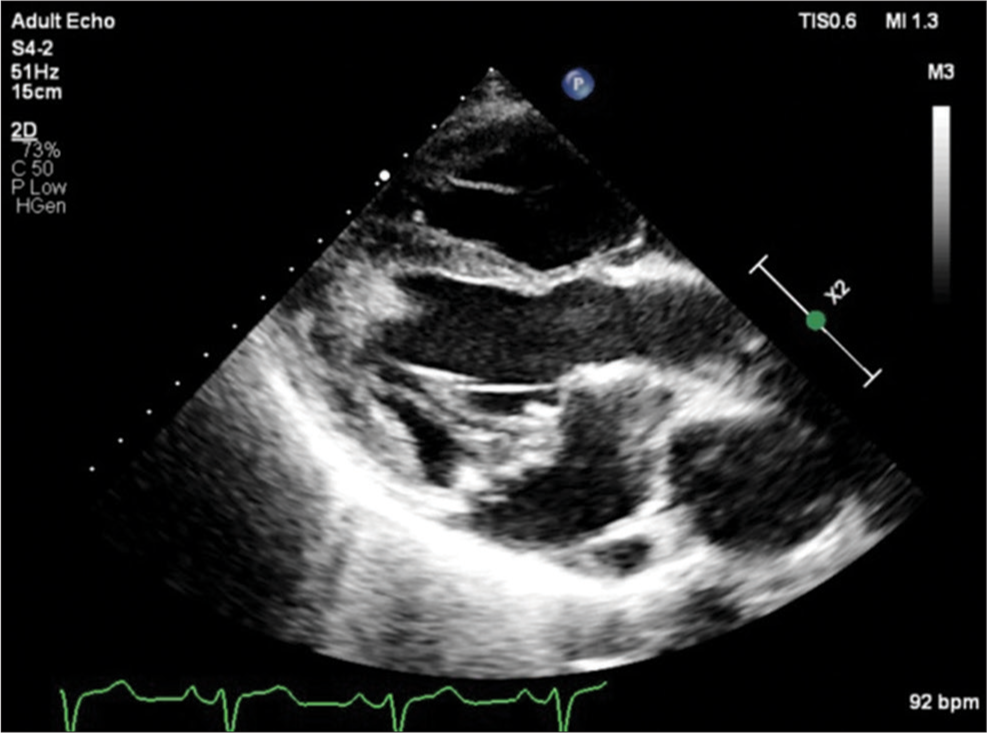
- Transthoracic echocardiogram parasternal long axis view showing mitral valve prolapse. P: Echocardiography probe orientation, X2: Two times magnified view.
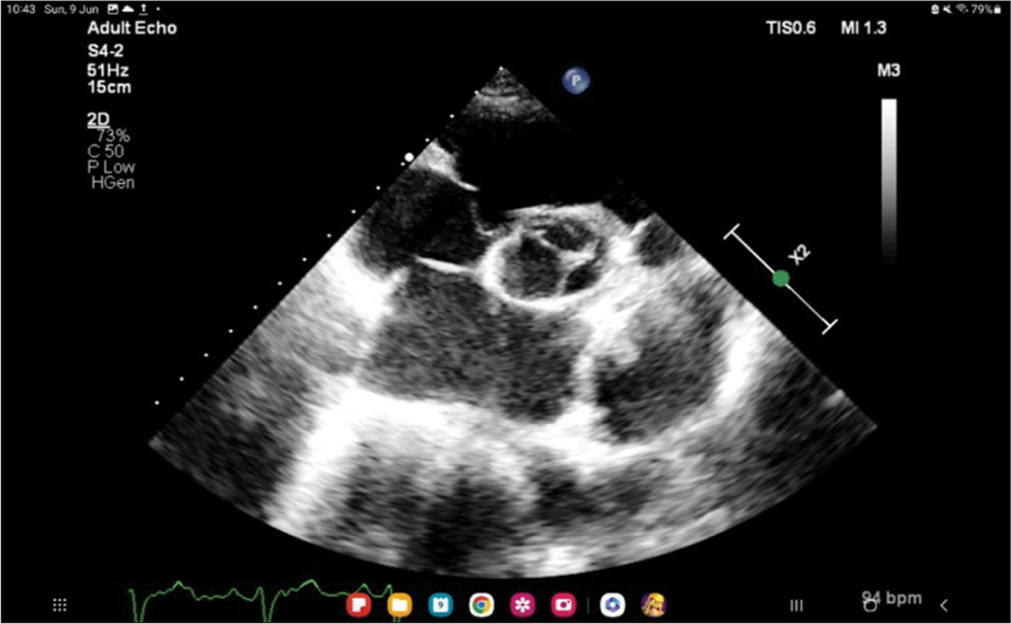
- Transthoracic echocardiogram parasternal short-axis view showing tricuspid valve prolapse. P: Echocardiography probe orientation, X2: Two times magnified view.
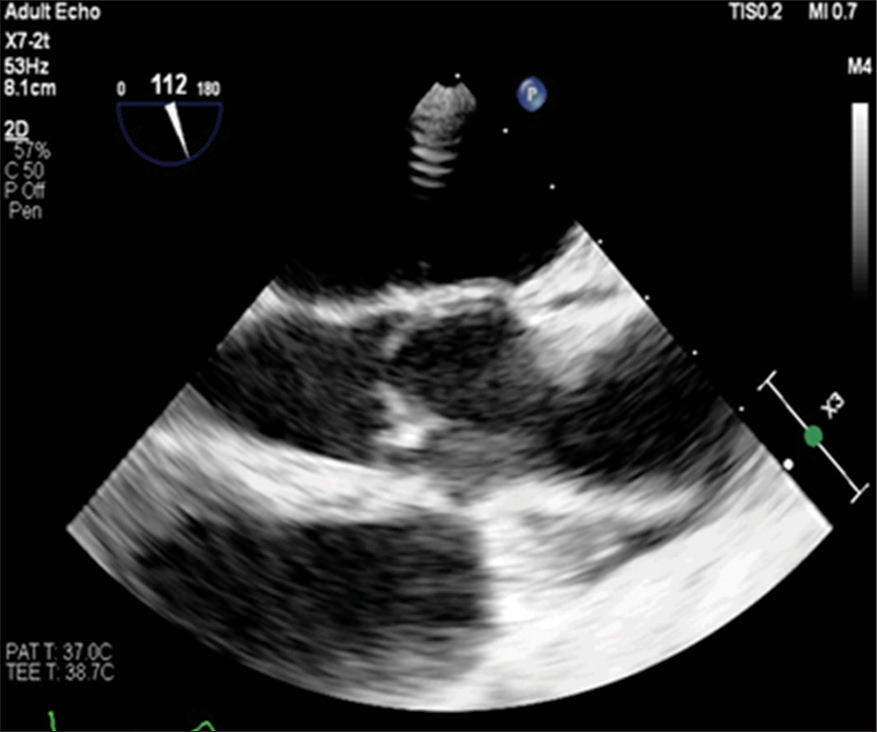
- Transesophageal echocardiography image showing aortic valve prolapse. P: Echocardiography probe orientation, X3: Three times magnified view.
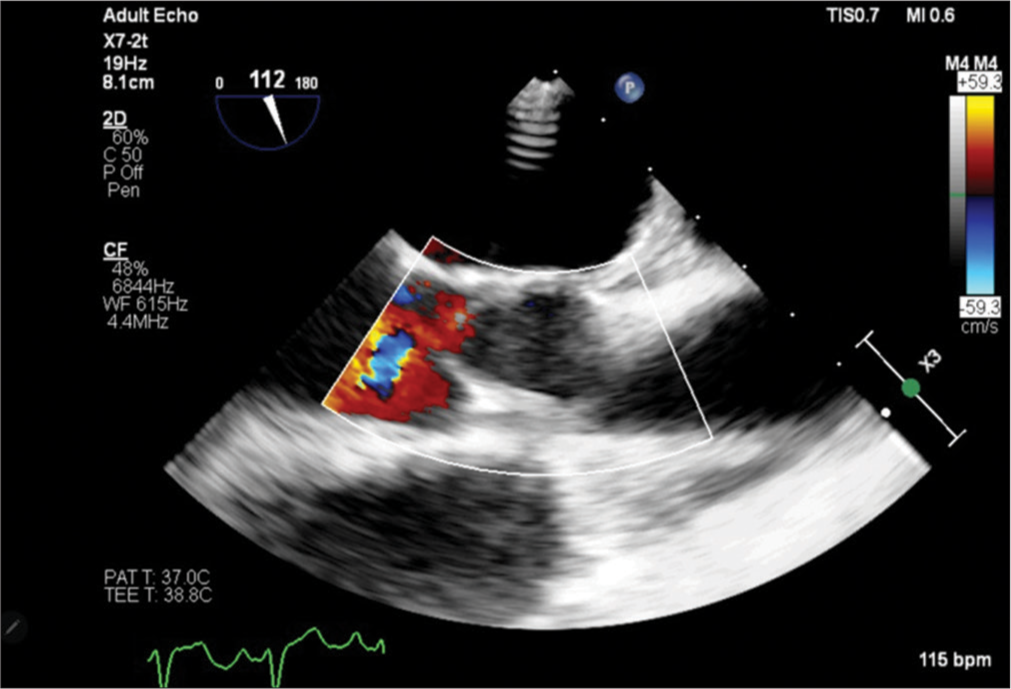
- Transesophageal echocardiography image showing aortic valve prolapse with aortic regurgitation. Colour flow imaging showing turbulent flow with mild regurgitant jet from prolapsed aortic valve. P: Echocardiography probe orientation, X3: Three times magnified view.
DISCUSSION
Myxomatous degeneration of cardiac valves is an uncommon finding, with their individual prevalence being 2–3% for isolated MVP in the general population.[8] Isolated TVP is rare, but in association with MVP, it is found in almost 50% of patients[9] whereas the prevalence of aortic valve prolapse is <1%.[3] However, multivalvular prolapse involving 3 or 4 valves is extremely rare. Clinical presentation of dyspnea, especially in the presence of confounding factors like smoking, can mislead to pulmonary diseases like COPD. In our case, the patient had symptoms spanning over several years but not being relieved with therapy. This highlights the importance of proper clinical examination in such patients, which can help in further deciding the line of evaluation.
Furthermore, in our case, TTE was done, which remains the cornerstone for the evaluation of multivalvular disease. But sometimes, few findings can be missed due to poor echocardiographic window in patients with concomitant pulmonary disease. Hence, TEE must be done in such cases which has better diagnostic accuracy.
Management of patients with multivalvular disease depends on possible changes in severity after treatment, the life expectancy and comorbidities, the individual surgical risk profile, the possibility of repair, the increased risk of redo surgery, and the feasibility of transcatheter approaches. Furthermore, there is a paucity of data on the natural history of multivalvular prolapse. This leads to difficulty in the management of such patients and requires further study in this field.
CONCLUSION
This is a case of multivalvular prolapse diagnosed on transthoracic echocardiograohy and confirmed on transesophageal echocardiography. Our case shows the importance of evaluation of all cardiac valves on echocardiography in a clinical suspected patient. Inspite of having symptomatic valvular regurgitant lesions, surgery was not possible due to increased surgical risk, so the patient was medically managed. This type of multivalvular patients requires comprehensive management by cardiologist and cardiac surgeons. Although myxomatous degenaration of cardiac valves suspected to be the cause of this valvular involvement, evaluation needs to be extended for other possible causes.
Author contributions
VG: Prepared the manuscript after compiling patient files and reports. MB: Proof reading of the manuscript and compiled images obtained on echocardiography. SDP: Proof corrections and overall patient evaluation.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Myxomatous degeneration of the mitral valve. Autops Case Rep. 2018;8:e2018058.
- [CrossRef] [PubMed] [Google Scholar]
- Echocardiographic determination of the prevalence of primary myxomatous degeneration of the cardiac valves. J Am Soc Echocardiogr. 2011;24:399-404.
- [CrossRef] [PubMed] [Google Scholar]
- An extremely rare case of isolated aortic valve prolapse causing aortic regurgitation in the absence of any other pre-existing cardiovascular or non-cardiovascular condition. Cureus. 2023;15:e46144.
- [CrossRef] [Google Scholar]
- Characteristics and significance of tricuspid valve prolapse in a large multidecade echocardiographic study. J Am Soc Echocardiogr. 2021;34:30-7.
- [CrossRef] [PubMed] [Google Scholar]
- Symptomatic valvular myxomatous transformation (the floppy valve syndrome). A possible forme fruste of the Marfan syndrome. Circulation. 1965;32:897-910.
- [CrossRef] [PubMed] [Google Scholar]
- An adult case with multiple cardiac valve prolapse and regurgitation. Intern Med. 1993;32:251-4.
- [CrossRef] [PubMed] [Google Scholar]
- Case report of multiple valve disease found in triplets. Twin Res Hum Genet. 2014;17:383-9.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. 1999;341:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and clinical implications of tricuspid valve prolapse based on magnetic resonance diagnostic criteria. J Am Coll Cardiol 2023:S0735-1097(22)07642-2.
- [Google Scholar]




