
Translate this page into:
Treatment outcomes in patients with multi-drug resistant tuberculosis

*Corresponding author: Unyime Israel Eshiet, Department of Clinical Pharmacy and Biopharmacy, University of Uyo, Uyo, Akwa Ibom, Nigeria. unyimeeshiet@uniuyo.edu.ng
-
Received: ,
Accepted: ,
How to cite this article: Eshiet UI, Akpan MR, Jackson IL, Uduak AS, Udiminue DS. Treatment outcomes in patients with multi-drug resistant tuberculosis. Med India. 2024;3:77-82. doi: 10.25259/MEDINDIA_18_2024
Abstract
Objectives:
The emergence of drug-resistant strains of Mycobacterium tuberculosis has substantially challenged the goal of eliminating tuberculosis (TB) in the 21st century. Treatment outcomes in patients with multi-drug resistant TB (MDR-TB) are expected to improve with the implementation of the World Health Organization consolidated guidelines for the treatment of MDR-TB. This study aimed to evaluate documented therapeutic outcomes in patients with MDR-TB treated at the University of Uyo Teaching Hospital, Nigeria.
Materials and Methods:
It was a retrospective study conducted at the MDR-TB unit of the University of Uyo Teaching Hospital, Nigeria. Data from case reports of patients with MDR-TB from 2013 to 2022 were extracted using a data collection checklist. Case reports with insufficient or missing information were excluded from the study. Data were summarized using the IBM Statistical Package for the Social Sciences version 25 (SPSS Inc., Chicago, USA).
Results:
Fifty case reports of patients with MDR-TB were evaluated. The most frequently prescribed anti-MDRTB drug combination was kanamycin, levofloxacin, pyrazinamide, prothionamide, cycloserine, and Vitamin B6 (n = 17; 34%). Weight gain was documented in 54% (n = 27) of the patients. Adverse events due to anti-MDR-TB medications was reported in 22% (n = 11) of the patients with ototoxicity (45.5%; n = 5) being the most frequently documented. Thirty-four (68%) of the patients were cured; 10 (20%) discontinued treatment; while 12% of the patients died.
Conclusion:
Although majority of the patients with MDR-TB treated at the University of Uyo Teaching Hospital were clinically cured, a significant proportion of the patients had poor treatment outcomes.
Keywords
Multi-drug resistant tuberculosis
Treatment
Outcomes

INTRODUCTION
Tuberculosis (TB) is an infectious disease and a leading cause of death globally. It is a disease of immense public health importance. In the year 2017, an estimated 10 million cases of the disease and 1.6 million deaths resulting from the disease was reported.[1,2] In spite of therapeutic advances that has brought a decline in deaths associated with the disease, TB remains a disease of public health importance as mortality from TB is still high.[3,4]
Usually, TB is treated pharmacotherapeutically using a combination of antibiotic regimen consisting of rifampicin, isoniazid, pyrazinamide, and ethambutol.[5] These drugs are widely used as first-line agents for TB. Unfortunately, over time, strains of Mycobacterium tuberculosis resistant to these drugs have emerged. The spread of drug-resistant TB has posed a great challenge to the global control of the disease. Patients who are infected with strains of the bacterium that is resistant to isoniazid and rifampicin, usually diagnosed as multi-drug resistant TB (MDR-TB) cannot be treated using the standard first-line treatment for TB as it would result in treatment failure.[4]
The emergence of drug-resistant strains of M. tuberculosis has substantially challenged the goal of eliminating TB in the 21st century. It poses a threat to TB control.[6] In 2017, the World Health Organization (WHO) reported an estimated 558,000 incidence of drug-resistant TB cases globally, with an estimated 3.5% of new TB cases and 18% of previously treated TB patients being diagnosed with MDR-TB in 2017.[1,2] Again, in 2018, the WHO reported a total of 186,772 cases of MDR-TB and 156,071 cases of rifampicin-resistant TB that initiated treatment globally. The organization also reported that approximately 3.4% of new TB cases and about 20% of patients with a history of previous treatment for TB were diagnosed with MDR-TB globally.[7,8]
The increase in the emergence and spread of MDR-TB has been attributed to poor treatment of TB. Patients with MDRTB are usually treated for a long duration (20–24 months) with second-line TB medications. Early detection of MDR-TB and prompt initiation of an effective treatment are critical factors in achieving successful therapeutic outcomes. In 2019, the WHO released a consolidated guideline for the treatment of MDR-TB. In these guidelines, the WHO suggested reclassification of second-line anti-TB drugs and recommended oral treatment regimens that included the new and repurposed agents. The WHO set a treatment target of 75–90% success rate for patients treated for MDR-TB.[1,7,8]
Advancement in technology and the introduction of newer agents such as bedaquiline, and repurposed drugs such as linezolid, clofazimine, and cycloserine as recommended by the WHO, is expected to improve treatment outcomes in MDR-TB patients.[7] The WHO treatment guideline is used in healthcare facilities managing patients with MDR-TB. Clinical outcome of care that includes cure rate among MDRTB patients can be used as an indicator for monitoring the success of these therapeutic interventions. In this study, we set out to assess therapeutic outcomes in patients with MDRTB receiving care at the University of Uyo Teaching Hospital, a referral tertiary healthcare facility in southern Nigeria.
MATERIALS AND METHODS
Research setting
This was a retrospective study conducted at the MDR-TB unit of the University of Uyo Teaching Hospital, a referral tertiary healthcare facility in southern Nigeria. Case notes of patients with MDR-TB treated at the University of Uyo Teaching Hospital, Nigeria, from 2013 to 2022 were extracted and reviewed.
Data on the sociodemographic and clinical characteristics of the patients were obtained using a data collection checklist. Data collected from the patients’ case notes included their gender, age, educational level, and presence of comorbidity. Furthermore, data on prescribed anti-MDR-TB medications, as well as documented clinical outcomes, were obtained. The clinical outcomes evaluated were as follows: documented adverse reactions associated with anti-MDR-TB medications, weight changes in patients, and the number of patients that were cured of MDR-TB.
The following operational definitions were used in assessing the outcome of treatment;
Cured: The treatment regimen was completed with no evidence of failure and three consecutive negative cultures taken at least 30 days apart
Treatment completed: The treatment regimen was completed without evidence of failure, but no record that three consecutive cultures taken at least 30 days apart are negative.
Treatment discontinued: The patients did not complete the treatment regimen.
Died: The patients who died during the course of MDRTB treatment.
Patients’ case notes were handled and treated with care. Data were collected and treated with utmost confidentiality.
Eligibility criteria
The eligibility criteria for the selection of case notes were case notes of the patients who were diagnosed with MDR-TB and received treatment at the University of Uyo Teaching Hospital, Nigeria. Case notes with insufficient or missing information were excluded from the study. The IBM Statistical Program and Service Solutions (Statistical Package for the Social Sciences) version 25.0 computer package was used to summarize data.
RESULTS
Sociodemographic details of the patients
Fifty case reports of patients with MDR-TB were evaluated. The majority of the cases studied were male (43; 86%), while 23 (46%) of the patients had comorbidities. The sociodemographic details of the patients are presented in Table 1.
| Parameters | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 43 | 86 |
| Female | 7 | 14 |
| Age range (years) | ||
| 10–30 | 18 | 36 |
| 31–50 | 22 | 44 |
| >50 | 10 | 20 |
| Educational level | ||
| Primary | 12 | 24 |
| Secondary | 20 | 40 |
| Tertiary | 8 | 20 |
| Informal education | 8 | 16 |
| Comorbidity | ||
| Present | 23 | 46 |
| Absent | 27 | 54 |
Pattern of utilization of anti-MDR-TB medications
The most frequently prescribed anti-MDR-TB drug combinations were kanamycin, levofloxacin, pyrazinamide, prothionamide, cycloserine, and Vitamin B6 (n = 17; 34%). The pattern of utilization of anti-MDR-TB medications is presented in Table 2.
| Anti-MDR-TB combination | Frequency | Percentage |
|---|---|---|
| Kanamycin/Levofloxacin/Pyrazinamide/Prothionamide/Cycloserine, and Vitamin B6. | 18 | 36 |
| Capreomycin/Moxifloxacin/Pyrazinamide/Prothionamide/Ethambutol/Isoniazid/Clofazimine/Vitamin B6. | 10 | 20 |
| Isoniazid/Ethambutol/Pyrazinamide/Moxiflozacin/Prothionamide/Bedaquiline/Cycloserine/Vitamin B6. | 4 | 8 |
| Kanamycin/Levofloxacin/Pyrazinamide/Ethionamide/Cycloserine/Vitamin B6. | 4 | 8 |
| Capreomycin/Levofloxacin/Pyrazinamide/Cycloserine/Vitamin B6. | 3 | 6 |
| Isoniazid/Pyrazinamide/Capreomycin/Moxifloxacin/Prothionamide/Clofazimine/B6. | 3 | 6 |
| Kanamycin/Clofazimine/Prothionamide/Moxifloacin/Pyrazinamide/Ethambutol/Isoniazide/B6. | 2 | 4 |
| Kanamycin/Levofloxacin/Prothionamide/Cycloserine/Vitamin B6. | 2 | 4 |
| Moxifloxacin/Pyrazinamide/Prothionamide/Ethionamide/Isoniazid/Clofazimine/Vitamin B6. | 2 | 4 |
| Ethambutol/Moxifloxacin/Clofazimine/Pyrazinamide/Capreomycin/Vitamin B6. | 1 | 2 |
| Cycloserine/Bedaquiline/Levofloxacin/Vitamin B6. | 1 | 2 |
MDR-TB: Multi-drug resistant-tuberculosis
Clinical outcomes of the cases studied
Adverse drug reaction (ADR) to anti-MDR-TB medications was documented in 22% (11) of the cases studied. Weight loss following treatment with MDR-TB medications was reported in 24% (12) of the cases studied, while 34 (68%) of the patients were cured following treatment with anti-MDR-TB medications. A graphical presentation of the documented ADR, weight changes, and number of patients cured of MDR-TB among the cases studied is presented in Figures 1-3, respectively.
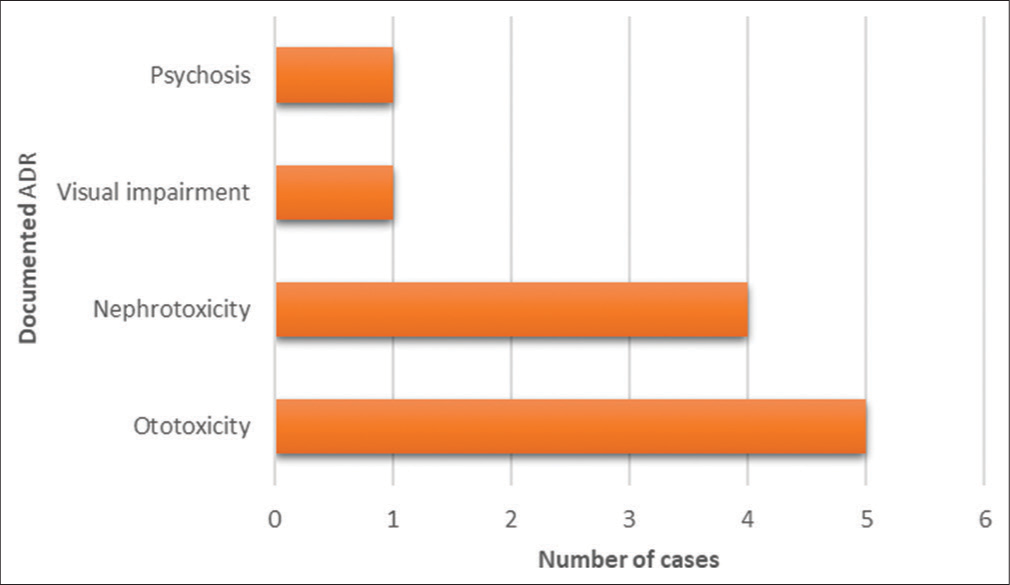
- Documented adverse drug reaction to anti-multi-drug resistant-tuberculosis medications.
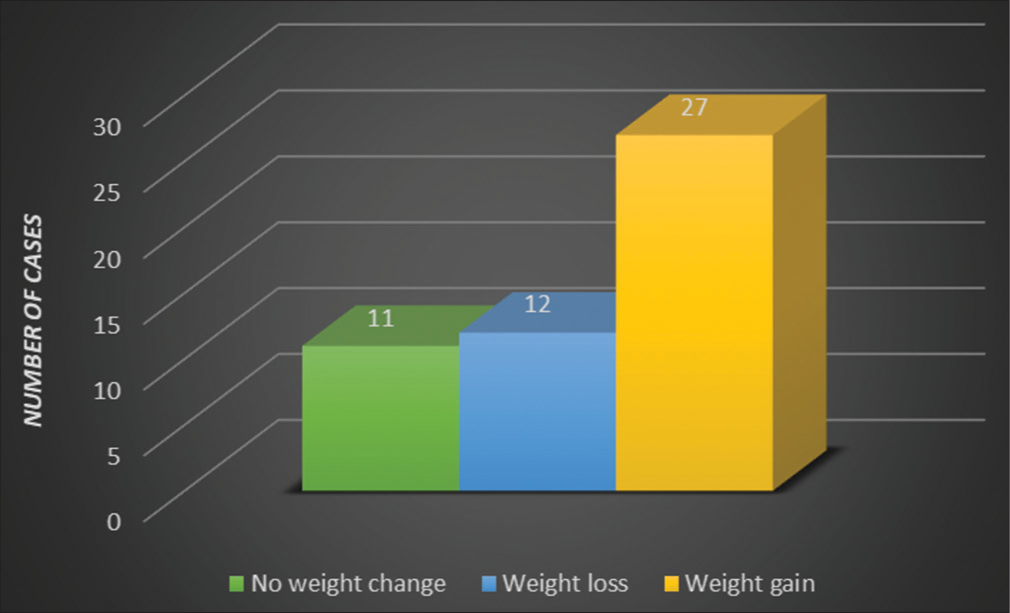
- Weight change following treatment with anti-multi-drug resistant-tuberculosis medications.
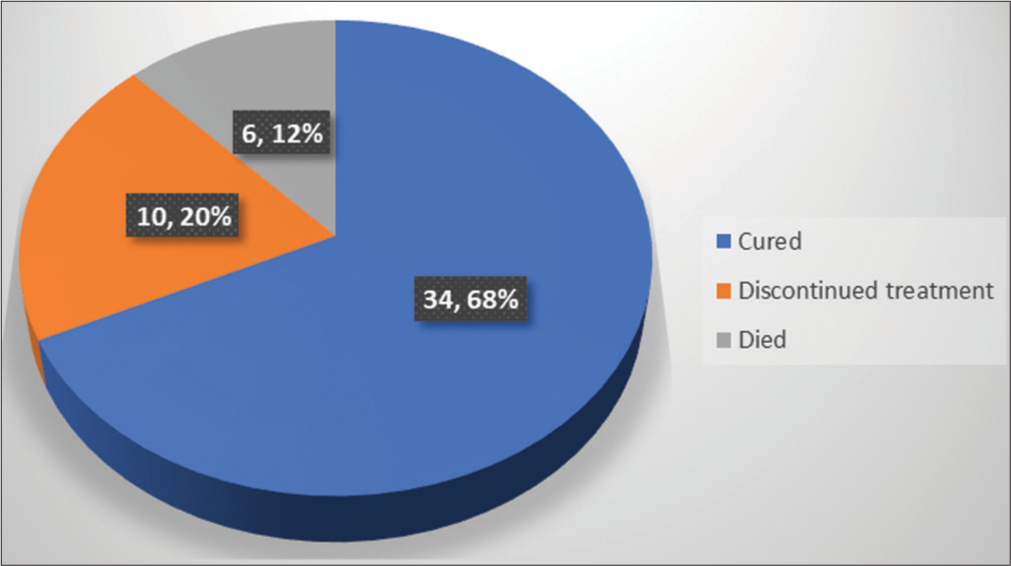
- Number of multi-drug resistant-tuberculosis cases cured following treatment.
DISCUSSION
MDR-TB is a fatal complication of TB and a condition of immense public health importance. It poses a serious threat to the health of members of the community. Our study was aimed at assessing the therapeutic outcomes of MDR-TB patients at the University of Uyo Teaching Hospital that was treated with the WHO recommended treatment regimen. We evaluated the documented adverse reactions associated with anti-MDR-TB medications, weight changes in the patients, and the number of patients who were cured of MDR-TB. Our findings showed that adverse reaction to anti-MDR-TB medications was documented in about one-fifth of the cases, with ototoxicity being the most frequently reported adverse effect associated with the use of these drugs. A similar study in China found that ADRs, which included hepatotoxicity and arthralgia, were documented in almost one-half of the cases.[9] Another study in India reported ADRs, including behavioral changes, ototoxicity, and musculoskeletal disorders among the MDR-TB cases studied.[10] Khan et al., in their study on MDR-TB patients, found that adverse drug effects (ADEs) of varying severity were reported in more than half of the patient population studied, with about one-quarter of the patients requiring modification of their anti-MDR-TB therapy.[11] A study among MDR-TB patients in referral hospitals in Ethiopia reported that the majority of the patients experienced at least one episode of ADRs during the course of treatment.[12] ADR is widely considered a major cause of medication non-adherence, which, in turn, affects treatment outcomes. It is believed to be the most important independent factor underlying non-compliance to pharmacological treatment.[11,13,14] It has been associated with therapeutic failure in patients with MDRTB.[9,15] History of khat use, presence of comorbidity, and long-term drug regimen have also been identified as possible predictors of major ADEs among MDR-TB patients.[16] Adequate management of the untoward effects of anti-MDRTB would significantly improve the outcomes of treatment. For instance, a prospective study on ADEs among patients with MDR-TB in Pakistan managed the ADEs using different measures, including modification of the therapeutic regimen, as well as the introduction of pharmacological, psychological, and supportive therapy.[11]
More than one-third of the cases of MDR-TB we studied had other co-existing medical conditions besides TB. A WHO report indicates that the presence of some comorbidity with MDR-TB increases the risk of adverse reactions to anti-MDR-TB medicines.[12] Furthermore, reports from similar studies in Nigeria and the United Kingdom show that the presence of any comorbidity with MDR-TB is associated with high mortality rates and poor treatment outcomes.[12,17]
We noted that weight loss during the course of treatment with anti-MDR-TB medicines was documented in about one-quarter of the cases studied. Weight loss has also been associated with an increased risk of ADEs in patients treated with anti-MDR-TB.[11] Previous research reports indicate that underweight patients are more prone to ADEs.[11,18,19] Low body mass index, weight loss, or insufficient weight gain during the course of treatment for MDR-TB increases the risk of ADRs and is associated with increased mortality.[12] Malnutrition impairs the recovery of patients with MDRTB and has been identified as a risk factor for low cure rates and increased death rates among poor patients living with MDR-TB.[12] Thus, clinicians should consider addressing malnutrition and improving patients’ body mass index as an important component of care for patients with MDR-TB. This is key to improving the treatment outcomes of these patients.[12]
On the other hand, weight gain can be used to evaluate patient response to anti-MDR-TB therapy, particularly in resource-limited settings.[20] MDR-TB patients with weight loss should be followed more closely, as they are at greater risk of death.[21] A study by Phan et al.[22] found that weight gain was associated with improvements in patients taking anti-TB therapy. They found that after 6 months of intensive phase, 62.4% of patients had gained at least 5% of their body weight, and those patients who did not gain up to 5% of their body weight had a linear increase in their weight over the treatment period. Thus, an increase in weight following therapy is usually accompanied by positive clinical outcomes. This is supported by a retrospective study by Chung-Delgado et al.[21] who found that patients who were eventually cured of MDR-TB after therapy gained 1.10 kg after the 1st month of therapy, in contrast to patients who died who lost 1.75 kg after the 1st month of therapy. Their study results revealed that patients who died did not gain any weight during the first 6 months of therapy. Hence, it is important for clinicians to evaluate patients who do not gain weight during the first few months of therapy, as this may be a pointer to poor treatment outcomes.[23]
About two-thirds of the cases we studied were cured following treatment with anti-MDR-TB medications. We also found that about one-quarter of the patients died during the course of treatment. A cure rate of at least 75% is considered an acceptable target for the treatment of patients with MDR-TB.[11] A cure rate of about 56% has been reported in previous studies.[11,24,25] Wakjira et al., in a similar study at referral hospitals in Ethiopia, reported a 69% composite treatment success rate and a 27% death rate among MDR-TB patients treated.[12] Other similar studies have reported treatment success rates ranging from 75% to 78.6%.[17,26,27]
The coexistence of certain chronic diseases with MDR-TB decreases the chances of recovery. For instance, the HIV co-infection with MDR-TB has been associated with a higher rate of death from MDR-TB.[27] In their report, Wakjira et al. attributed the high death rate found in their study to a high rate of MDR-TB and HIV/AIDS co-infection found among the patients included in their study.[12] On the other hand, Baluku et al. attributed the inability to achieve the desired cure rate among MDR-TB patients to the high cost of MDR-TB therapy, the lower efficacy of these drugs, and the increased incidence of adverse effects (which affects patients’ medication adherence) when compared to first-line therapy used for medication-susceptible TB.[24]
Limitations
This was a cross-sectional study; thus, causal links could not be established due to a lack of temporal connections. Furthermore, the study was based on a review of medical records; thus, the study design and findings were limited to what was documented in the case notes.
CONCLUSION
Although a majority of the patients with MDR-TB treated at the University of Uyo Teaching Hospital were clinically cured, a significant proportion of the patients had poor treatment outcomes. Weight loss and ADR were reported in a significant proportion of the cases studied. There is a need for clinicians to identify the factors determining treatment outcomes of patients with MDR-TB. This would help in implementing decisive measures to improve the outcome of care for these patients.
Author contributions
UE: Principal investigator, conception, study design, data collection, data analysis/interpretation, draft article, and critical review of final manuscript; MA: Data analysis/interpretation, draft article and critical review of final manuscript; IJ: Data collection, data analysis/interpretation, draft article; AU: Data collection, data analysis/interpretation and draft article, and critical review of final manuscript; DU: Data collection, data analysis/interpretation and draft article.
Ethical approval
The research/study was approved by the Institutional Review Board at the University of Uyo Teaching Hospital, Nigeria, number UUTH/AD/S/96/VOL.XXI/666, dated May 23, 2022.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Treatment outcomes of multi drug resistant and rifampicin resistant Tuberculosis in Zimbabwe: A cohort analysis of patients initiated on treatment during 2010 to 2015. PLoS One. 2020;15:e0230848.
- [CrossRef] [PubMed] [Google Scholar]
- Global tuberculosis report 2018. 2018. Geneva, Switzerland: WHO; Available from: https://www.who.int/publications/i/item/9789241565646 [Last accessed on 2023 Dec 27]
- [Google Scholar]
- The history of tuberculosis: From the first historical records to the isolation of Koch's bacillus. J Prev Med Hyg. 2017;58:E9-12.
- [Google Scholar]
- Global tuberculosis report 2021. 2018. Geneva, Switzerland: WHO; Available from: https://www.who.int/publications/digital/global-tuberculosis-report-2021 [Last accessed on 2024 Jan 02]
- [Google Scholar]
- Evolution of drug-resistant Mycobacterium tuberculosis strains and their adaptation to the human lung environment. Front Microbiol. 2021;12:612675.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment effectiveness and outcome in patients with a relapse and newly diagnosed multidrug-resistant pulmonary tuberculosis. Med Glas (Zenica). 2020;17:356-62.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of multidrug-resistant tuberculosis. Yeungnam Univ J Med. 2020;37:277-85.
- [CrossRef] [PubMed] [Google Scholar]
- Global tuberculosis report 2019. 2019. Geneva, Switzerland: WHO; Available from: https://iris.who.int/bitstream/handle/10665/329368/9789241565714-eng.pdf?sequence=19 [Last accessed on 2024 Jan 05]
- [Google Scholar]
- Treatment outcomes of patients with multidrug and extensively drug-resistant tuberculosis in Zhejiang, China. Eur J Med Res. 2021;26:31.
- [CrossRef] [PubMed] [Google Scholar]
- Trends and treatment outcomes of multidrug-resistant tuberculosis in Delhi, India (2009-2014): A retrospective record-based study. Indian J Med Res. 2020;151:598-603.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of adverse drug events, their risk factors, and management among patients treated for multidrug-resistant TB: A prospective cohort study from Pakistan. Front Pharmacol. 2022;13:876955.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment outcomes of patients with MDR-TB and its determinants at referral hospitals in Ethiopia. PLoS One. 2022;17:e0262318.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence and predictors of major adverse drug events among drug-resistant tuberculosis patients on second-line anti-tuberculosis treatment in Amhara regional state public hospitals; Ethiopia: A retrospective cohort study. BMC Infect Dis. 2019;19:286-312.
- [CrossRef] [PubMed] [Google Scholar]
- Adverse drug reaction profile of daily regimen antituberculosis treatment. Perspect Clin Res. 2022;13:194-8.
- [CrossRef] [PubMed] [Google Scholar]
- Serious treatment related adverse drug reactions amongst anti-retroviral naive MDR-TB patients. PLoS One. 2013;8:e58817.
- [CrossRef] [PubMed] [Google Scholar]
- A score to predict the risk of major adverse drug reactions among multi-drug resistant tuberculosis patients in Southern Ethiopia, 2014-2019. Infect Drug Resist. 2022;15:2055-65.
- [CrossRef] [PubMed] [Google Scholar]
- Transmission of multidrug resistant tuberculosis in the UK: A cross sectional molecular and epidemiological study of clustering and contact tracing. Lancet Infect Dis. 2014;14:406-15.
- [CrossRef] [PubMed] [Google Scholar]
- Adverse drug reactions of anti-tuberculosis treatment among children with tuberculosis. Int J Mycobacteriol. 2020;9:281-8.
- [CrossRef] [PubMed] [Google Scholar]
- Adverse events associated with treatment of multidrug-resistant tuberculosis in China: An ambispective cohort study. Med Sci Monit. 2017;23:2348-56.
- [CrossRef] [PubMed] [Google Scholar]
- Weight gain and response to treatment for multidrug-resistant tuberculosis. Am J Trop Med Hyg. 2013;89:943-9.
- [CrossRef] [PubMed] [Google Scholar]
- Weight variation over time and its relevance among multidrug-resistant tuberculosis patients. Int J Infect Dis. 2014;23:20-4.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors and patterns of weight gain during treatment for tuberculosis in the United States of America. Int J Infect Dis. 2016;53:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- Weight variation over time and its association with tuberculosis treatment outcome: A longitudinal analysis. PLoS One. 2011;6:e18474.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment outcomes of drug resistant tuberculosis patients with multiple poor prognostic indicators in Uganda: A countrywide 5-year retrospective study. J Clin Tuberc Other Mycobact Dis. 2021;23:100221-8.
- [CrossRef] [PubMed] [Google Scholar]
- Side effects associated with the treatment of multidrug-resistant tuberculosis at a tuberculosis referral hospital in South Korea: A retrospective study. Medicine (Baltimore). 2017;96:E7482-6.
- [CrossRef] [PubMed] [Google Scholar]
- The experience of scaling up a decentralized, ambulatory model of care for management of multidrug-resistant tuberculosis in two regions of Ethiopia. J Clin Tuberc Other Mycobact Dis. 2017;7:28-33.
- [CrossRef] [PubMed] [Google Scholar]
- Achieving high treatment success for multidrug-resistant TB in Africa: Initiation and scale-up of MDR-TB care in Ethiopia-an observational cohort study. Thorax. 2015;70:1181-8.
- [CrossRef] [PubMed] [Google Scholar]




