
Translate this page into:
Lentil hypersensitivity pneumonitis as a masquerader in an infant with recurrent pneumonia

*Corresponding author: Vijay Ganesh, Junior Resident, Department of Pediatrics, Base Hospital Delhi Cantt, New Delhi, India. vijay.bg.ganesh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Balasubramania S, Ganesh V, Pathania A, Taneja M. Lentil hypersensitivity pneumonitis as a masquerader in an infant with recurrent pneumonia. Med India. 2024;3:94-8. doi: 10.25259/MEDINDIA_22_2024
Abstract
Lentils appear to be the most frequent legume associated with childhood allergies in the Mediterranean and India. The prevalence of food-allergic diseases in childhood is around 3%, with a range between 1.4-4% for common allergens. The Papilionaceae family, which includes legumes such as lentils, chickpeas, green beans, peanuts, and soy, is a significant part of the European diet. These foods are among the top five causes of immunoglobulin E-mediated allergic reactions. These allergies often begin early, before the age of four. Hypersensitivity pneumonitis (HP) causes a different immune reaction in your body than pollen or pet allergies. Unlike common allergies that cause hay fever and asthma, repeated exposure to allergens that cause HP can lead to inflammation that can permanently damage your lungs. We report a case of an infant who developed HP after recurrent aspiration/inhalation of lentils.
Keywords
Allergy
Immunology
Pediatric
Hypersensitivity pneumonitis
Gastroesophageal reflux disease

INTRODUCTION
Infants presenting with atypical pneumonia are common. While infective etiology is often investigated, hypersensitivity pneumonitis (HP) is seldom evaluated.[1,2] The key to early detection is early suspicion of hypersensitivity. Here, we describe an infant with recurrent pneumonia who, despite initial management,[3] had persisting symptoms, prompting further evaluation for hypersensitivity. While less common than allergies to peanuts or soy, lentil hypersensitivity is becoming increasingly recognized, particularly in certain regions.[4] HP due to lentils is a specific type of lung inflammation caused by inhaling/aspiration of lentil dust or particles. While less common than other forms of lentil allergies, it is important to understand its unique characteristics and potential risks.
CASE REPORT
This one-year-old, firstborn of non-consanguineous marriage, developmentally normal infant presented with a history of recurrent episodes of bronchitis and conjunctivitis during the spring period, failure to thrive with height and weight <3 standard deviation (SD). Antenatal and birth history were unremarkable. There was no history of contact with tuberculosis (TB), recurrent diarrhea, oily stool, recurrent ear discharge, food allergy, or exposure to pigeons. There was no history of indoor pollution and smoking in the family or any early sibling deaths. The child started on weaning foods, including wheat, rice, and lentils, at 6–8 months with a history of vomiting post-feed frequently and forced feeding. The infant had repeated hospital visits for the same and was managed conservatively. Despite repeated medications (antibiotics and anti-gastroesophageal reflex [GER] measures), the infant had transient asymptomatic phases. He had failure to thrive despite these measures and persistent forceful feeding habits.
On arrival at this tertiary care hospital with features of pneumonia (tachypnea and cough), the baby was thoroughly investigated with initial differentials of primary immunodeficiency, protracted bacterial bronchitis, and GER disease and started along with a short course of antibiotics for a two-week duration. The investigations are attached as per Table 1. The radionucleotide milk scan was positive for GER grade 2 [Figure 1]. Chest X-ray was suggestive of bilateral perihilar opacities indicating recurrent micro aspirations [Figure 2], and contrast-enhanced computed tomography chest showed peri bronchial consolidation predominantly involving the upper and middle lobes. Bronchoalveolar lavage (BAL) revealed predominant lymphocytes with eosinophils, and BAL GeneXpert for TB was negative. In view of the characteristic features of HP, further workup considering lentil hypersensitivity was done which was serum immunoglobulin E (IgE). Lentil Ag was raised by 22.1 kilounits/litre (kUA/L); normal range <0.1 kUA/lt. Prick tests confirmed an allergy to lentils but were negative for other common food allergens.
| Tests | Results | Normal value |
|---|---|---|
| Complete cell count | ||
| Hb (g/dL) | 9.6 | 11.5–13.5 |
| Total leukocyte count (×109/L) | 8.8 | 9–11 |
| Differential leukocyte count (DLC) | Neutrophils (N) 17%, Lymphocytes (L) 64%, Monocytes (M) 8%, Eosinophils (E) 1% | |
| Platelet count (×109/L) | 219 | 150–450 |
| Peripheral blood film | DLC: N 40, L 50, M 9, E 1. No Tg, Tv. No atypical cells. Platelet-adequate | |
| Biochemistry | ||
| Blood urea nitrogen (mg/dL) | 4 | <45 |
| Serum creatinine (mg/dL) | 0.3 | <0.7 |
| Bilirubin (mg/dL) | Total-1.0, Direct- 0.5 | 0.3–0.5 |
| Aspartate transaminase (IU/L) | 31 | 0–45 |
| Alanine transferase (IU/L) | 35 | 0–50 |
| Alkaline Phosphatase (IU/L) | 210 | <400 |
| Lactate dehydrogenase (IU/L) | 154 | 240-480 |
| Triglycerides (mg/dL) | 124 | <150 |
| Investigations for cause | ||
| CRP (mg/dL) | 13.3 | <5 |
| Procalcitonin | 0.1 | <0.1 |
| Erythrocyte Sedimentation Rate (mm/hr) | 11 | 8-11 |
| Ferritin | 15 | |
| Fibrinogen (g/L) | 1.2 | 2-4 |
| Blood culture | No growth | |
| Gastric aspirate acid–fast bacilli and mycobacterial tuberculosis (GeneXpert) | Negative | |
| Truenat MTB | Not detected | |
| C3 level (g/L) | 0.94 | 1–1.9 |
| Immunoglobulin G (mg/dL) | 1649 | 500–2000 |
| Immunoglobulin A (mg/dL) | 52.50 | 50–100 |
| Immunoglobulin M (mg/dL) | 247 | <200 |
| Miscellaneous | ||
| USG abdomen | Normal study, no organomegaly | |
| X-ray Chest | Bilateral perihilar opacities | |
CRP: C-reactive protein, MTB: Mycobacterium tuberculosis, USG: Ultrasound sonography, Hb: Hemoglobin, Tg- Toxic grandules, Tv- Toxic vesicles
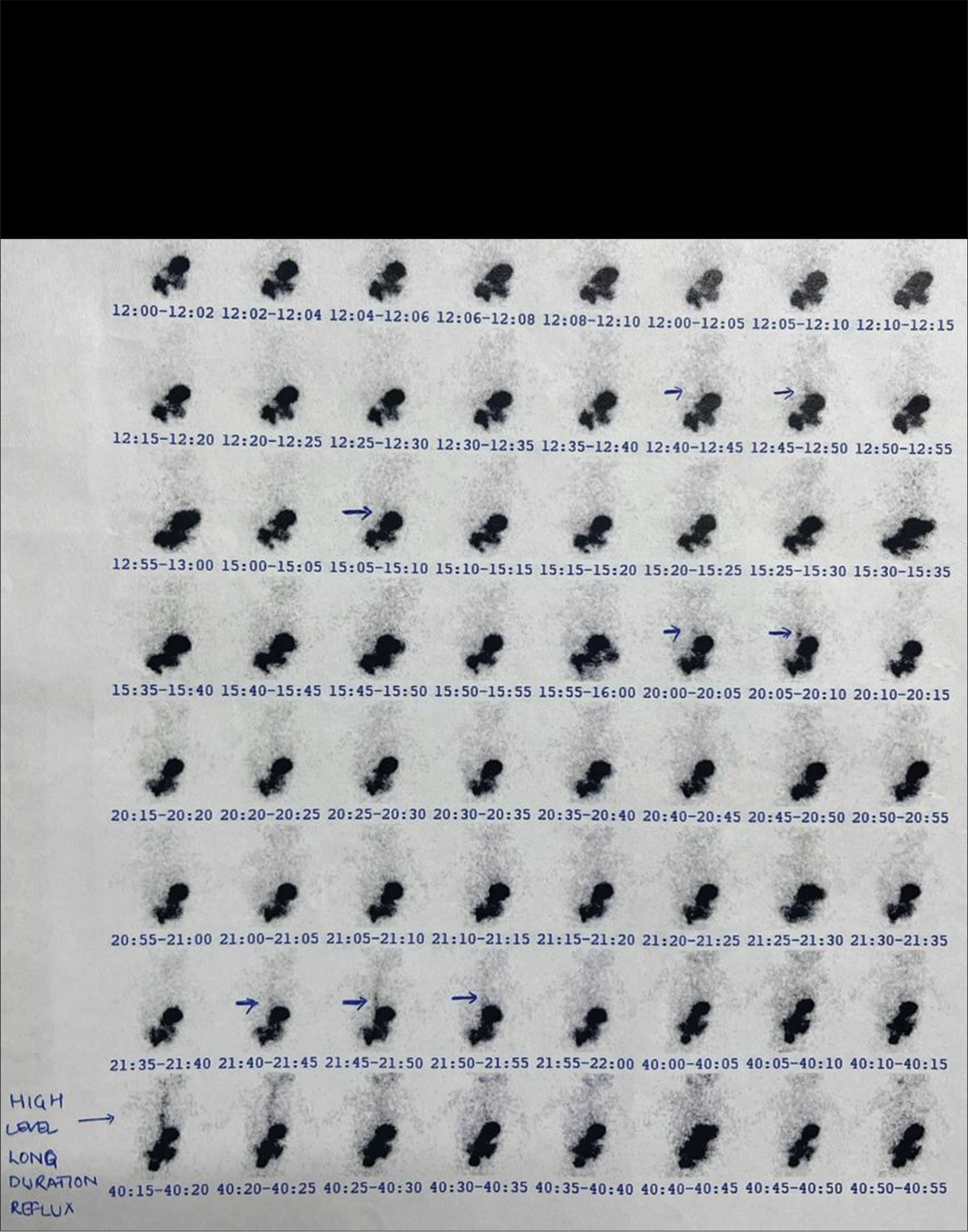
- Gastroesophageal reflux scan; high reflux noted.

- Chest X-ray posteroanterior view showing peribronchial opacities suggestive of microaspirations.
Management
The baby was placed on a lentil-free diet initially and started on low-dose inhalational corticosteroids and antihistamines along with proton pump inhibitors with position and technique of breastfeeding and complimentary diet. On the first review, the infant had subjective improvement and had no signs of respiratory symptoms. The infant was later weaned off of inhalational corticosteroids over a period of four weeks and continued on a lentil-free diet. The plan to reintroduction of diet in smaller proportions is in progress.
DISCUSSION
Hypersensitive pneumonitis is one of the leading interstitial lung diseases in children, with a prevalence of 4 in 1 million.[5] The common manifestations of HP are non-specific and include cough, fever, tachypnea, or respiratory distress. At present, there are no diagnostic criteria for HP in the pediatric population and respiratory symptoms; the high-resolution computed tomography findings are helpful in establishing the diagnosis.[5] BAL and lung biopsy have added diagnostic values but may not always be necessary when the history of exposure and typical radiological findings are conspicuous. Lentils are grown in many temperate and subtropical regions worldwide. While they are commonly eaten, there is limited information in literature about severe allergic reactions, like anaphylaxis, caused by consuming them.[4] The growing number of reported lentil allergies has led to research into how lentils might cause allergic reactions. Two types of allergens have been identified in boiled lentils. These allergens are proteins L1, L2 (both 16 kDa), and L3 (12 kDa), which are related based on their structure and immune properties. Protein L1 was found to be a significant allergen in lentil allergy. This was supported by its high recognition rate (68%) by patient sera and its ability to inhibit (64%) IgE binding to commercial lentil allergen extracts.[6] The second allergen identified in boiled lentils is protein H, a 66 kDa component that binds to IgE. Purified protein H was recognized by 41% of patient sera and inhibited IgE binding to commercial lentil extracts by 45%. Boiling lentils appears to break down existing allergens into smaller fragments, which may have stronger allergenic properties.[7] The most likely explanation for these allergic reactions is IgE-mediated hypersensitivity. This occurs when a person’s immune system becomes sensitized to a food after eating it and then reacts to it through an IgE-mediated response.[8]
As a result, the person may experience symptoms even after simply inhaling the vapors from boiling food, similar to what happens in inhalant allergies, with clinical manifestations involving various organs such as the lungs and skin, and even evolving in anaphylaxis. In our index case, the hypersensitivity might be primarily due to increased aspirations due to GER. Unlike previous cases, our patient experienced very early symptoms, starting before the age of one. There are no reported cases of anaphylaxis in children so young, especially when they are already on a lentil-free diet.
Our case highlights that a strict diet may not always prevent allergic reactions, and these reactions can occur even after inhaling cooking vapors. Although rare, this risk should be considered in children who have a food allergy, even if they follow an exclusion diet.
CONCLUSION
HP is an immune-mediated inflammatory reaction that affects the lungs. HP due to lentils is a specific type of lung inflammation caused by inhaling lentil dust or particles. It is distinct from the more common food allergy to lentils, where the reaction occurs through ingestion.
Inhaling lentil dust or particles triggers an abnormal immune response, leading to inflammation and damage to the lung tissue.
This can cause a range of symptoms, from mild cough and shortness of breath to severe respiratory distress.
Early identification and dietary management, combined with targeted interventions like steroids in severe cases, can lead to significant improvement in patient outcomes and prevent the progression of disease to chronic lung disease. The key to early diagnosis lies in early suspicion of hypersensitivity, especially in weaning infants who are force-fed and/or neurologically compromised. This case highlights the potential for severe reactions to lentils, even in previously unexposed individuals. Early recognition and intervention are crucial in anaphylaxis management. Parents and healthcare professionals must be aware of this emerging allergy and have a low threshold for suspicion.
Author contributions
SB: Prepared the manuscript after compiling patient files and reports; AP: Drafting the work or reviewing it critically for important intellectual content; VG: Proof reading of the manuscript; MT: Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The prevalence of food allergy: A meta-analysis. J Allergy Clin Immunol. 2007;120:638-46.
- [CrossRef] [PubMed] [Google Scholar]
- Atopic disease, immune system and environment: Which linkage? Allergy Asthma Proc. 2007;28:410-7.
- [CrossRef] [PubMed] [Google Scholar]
- Allergy to lentils in Mediterranean pediatric patients. J Allergy Clin Immunol. 1999;103:154-8.
- [CrossRef] [PubMed] [Google Scholar]
- Paediatric hypersensitivity pneumonitis: Literature update and proposal of a diagnostic algorithm. Ital J Pediatr. 2022;48:51.
- [CrossRef] [PubMed] [Google Scholar]
- The vicilin gene family of pea (Pisum sativum L.): A complete cDNA coding sequence for preprovicilin. Nucl Acids Res. 1983;11:2367-80.
- [CrossRef] [PubMed] [Google Scholar]
- Identification and cloning of a complementary DNA encoding a vicilin-like proprotein, Jug r 2, from English walnut kernel (Juglans regia), a major food allergen. J Allergy Clin Immunol. 1999;104:1311-20.
- [CrossRef] [PubMed] [Google Scholar]
- Food allergy and probiotics in childhood. J Clin Gastroenterol. 2010;44:22-5.
- [CrossRef] [PubMed] [Google Scholar]




