
Translate this page into:
A comparison of Delta and Omicron waves of COVID-19 pandemic: An observation from a tertiary care center from North India

*Corresponding author: Dr. Peetam Singh. Department of Microbiology, Subharti Medical College, Meerut, Uttar Pradesh, India. kgmclko@gmail.com
-
Received: ,
Accepted: ,
This article has been Retracted, Retraction Notice available at 10.25259/MEDINDIA_4_2024
How to cite this article: Shukla S, Singh P. A comparison of delta and Omicron waves of COVID-19 pandemic: An observation from a tertiary care center from North India. Med India 2023;2:16.
Abstract
Objectives:
The impact of the Omicron variant (B.1.1.529) was very low as compared to the Delta variant (B.1.617.2) in North India. Very few studies are there highlighting the clinical parameters associated with disease outcomes among coronavirus disease-2019 (COVID-19) patients during the Delta and Omicron waves of the pandemic. This study was conducted to observe various clinical parameters associated with disease outcomes among COVID-19 patients during Delta and Omicron waves.
Materials and Methods:
This retrospective observational study was conducted during the Delta wave (March 2021 to June 2021) and Omicron wave (December 2021 to March 2022) on patients with positive reverse transcriptase–polymerase chain reaction (RT-PCR) admitted during the study period. The patient characteristics and outcome measures including demographic, baseline clinical, disease severity, intensive care unit admissions, and hospital mortality were recorded.
Results:
Out of total of 1731 patients who tested positive for severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) by RT-PCR, 16 patients were admitted during the omicron wave and 878 were admitted during the Delta wave. The majority of admitted patients during the Delta wave were in the age groups of 21–40 and 41–60 years, with significantly less number of admissions in the age group of <20 years during the Omicron wave. The admissions were significantly lower during the Omicron wave (P < 0.001). Patients without a previous history of COVID-19 and unvaccinated status were having significantly higher admissions (P < 0.001). During Delta and Omicron waves 71.4% and 18.75% of the patients, respectively, were having no comorbidities.
Conclusion:
Hospital admissions were higher during the Delta wave in comparison to the Omicron wave. During the Delta wave, the degree of severity and number of deaths were also very high.
Keywords
Delta variant
Omicron variant
SARS-CoV-2 variants
Variants of concern
COVID-19

INTRODUCTION
The wild strain of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the Wuhan variant, has now emerged into a variety of variants. Based on the impact of mutations in SARS-CoV-2 on the effectiveness of the medical countermeasure, severity of disease, and ability to spread from person to person, the World Health Organization (WHO) has divided them into three categories including variants of concern (VOCs), variants of interest and variants under monitoring. The VOCs designated previously by WHO are Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2) due to which many people around the world have been infected and died.[1] For the 1st time, the Delta variant (B.1.617.2) was detected in India in the month of March 2021 which was the result of 13 different mutations in SARS-CoV-2.[2] More than 80 countries around the world were soon affected due to the high transmission rate of the Delta variant. The morbidity and mortality due to the Delta variant were also very high around the globe.[3]
Another SARS-CoV-2 variant B.1.1.529, which is now referred to as the Omicron variant by WHO is the fifth VOC and was first identified in South Africa in November 2021.[4] The Omicron variant has been reported to be the result of around 50 mutations in the genome of SARS-CoV-2 of which 30 are present in spike protein.[5] In India, the first Omicron variant was identified in Karnataka on November 25, 2021, and within 20 days, India had reported approximately 200 cases of Omicron. The current concern is that Omicron can evade immunity induced by the currently used vaccines and drugs.[3]
Outlining the transmission of the Omicron at this time is scanty and an evaluation is required for the effectual control of this variant worldwide. It is important to explore whether the transmission rate and symptoms of the Omicron variant can be attributed to immune evasiveness. Some studies have shown that infection with the Omicron variant has been seen even in people who have received two full doses of coronavirus disease-2019 (COVID-19) vaccines.[6] It has been found that the chances of infection have decreased in people who have taken all doses of vaccination and if there was an infection, most of them have been cured by home isolation or with a shorter duration of hospitalization.[7,8]
The focus of this study was to explore the factors that played a role in admission and patient outcomes during the Delta and Omicron waves.
MATERIALS AND METHODS
This retrospective observational study was conducted at a tertiary care hospital in Uttar Pradesh, India. In this study, reverse transcriptase–polymerase chain reaction (RT-PCR) positive for COVID-19 patients of all age groups admitted during the study period were included in the study. The patients who were admitted with the symptoms and signs of COVID-19 but found negative for COVID-19 on RT-PCR were excluded from the study.
The main objective of this study was to compare age group, gender, patient community, past history of COVID-19, associated comorbidities, vaccination status, intensive care unit (ICU) admissions, disease severity, and outcomes. Data of patients admitted during the Delta wave (March 1, 2021, to June 30, 2021) and Omicron wave (December 26, 2021, to March 20, 2022), on epidemiology, patient demography, clinical, and outcome parameters were extracted from patient history data available in hospital records. History related to COVID-19 vaccination, previous history of COVID-19, and clinical profiles of patients such as body temperature, degree of severity, underlying comorbidities, duration of hospital stay, and outcome of patients were noted.
RT-PCR was done in our COVID-19 testing laboratory as per the manufacturer’s instructions targeting the envelope, open reading frame 1b, and RNA-dependent RNA polymerase genes of beta coronavirus and SARS-CoV-2. RT-PCR-positive samples were stored and sent to the Central Drug Research Institute, Lucknow, for whole-genome sequencing to know the SARS-CoV-2 variants.
The most commonly observed mutations were found in the spike protein of SARS-CoV-2 virus, which were Spike_ D796Y, Spike_D614G, Spike_N969K, Spike_N764K, and Spike_Q954Y, whereas two mutations of Spike_K417N and Spike_W258L were observed in the spike protein in the Delta variants from this region.[9]
Statistical analysis
Categorical variables were presented as frequency and percentages (n; %). Statistical analysis was done using the Statistical Package for the Social Sciences software version 26 (IBM Corp., Armonk, NY, USA). The comparability of groups was analyzed by Chi-square and P-value. Interpretation was done considering P < 0.05 as statistically significant.
RESULTS
In our study, a total of 1731 patients were found to be positive by RT-PCR for SARS-CoV-2 during the study period. Among all positive cases, 1153 and 578 cases were registered during Delta and Omicron waves, respectively. There were 65% and 74% males during the Delta and Omicron waves, respectively, without any significant difference.
All 16 samples from admitted patients were identified as Omicron variant during the Omicron wave. We compared the 16 patients admitted during the Omicron wave with 878 admissions during the Delta wave [Figure 1].
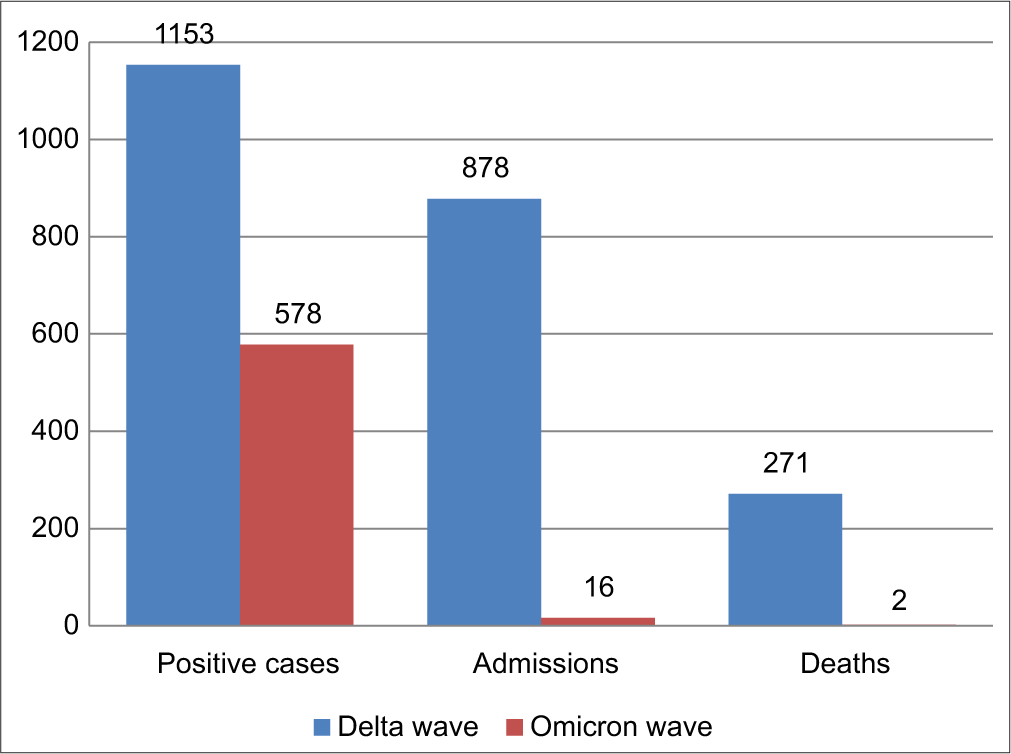
- Comparison of COVID-19 cases during Delta and Omicron waves.
The majority of admitted patients during the Delta wave were in the age groups of 21–40 and 41–60 years, with significantly less number of admissions in the age group of <20 years during the Omicron wave. The admissions were significantly lower during the Omicron wave (P < 0.001). Patients without a previous history of COVID-19 and unvaccinated status had significantly higher admissions (P < 0.001). During Delta and Omicron waves, 71.4% and 18.75% of the patients, respectively, were having no comorbidities. Whereas in the remaining patients, one or more comorbidities were found but the numbers were again very low during the Omicron wave. The admission rate among patients having comorbidities was also significantly low during the Omicron wave (P < 0.001) [Table 1].
| Indicators | Delta (2nd) wave; n (%) | Omicron (3rd) wave; n (%) | P-value |
|---|---|---|---|
| COVID-19 cases | |||
| Total | 1153 | 536 | <0.001* |
| Admitted | 878 (76.1) | 16 (3.0) | |
| Mean age | 46.8 | 49.25 | |
| Age group | |||
| 0–20 | 51 (6.3) | 1 (0.06) | <0.001* |
| 21–40 | 290 (33) | 4 (30.8) | |
| 41–60 | 352 (39) | 4 (30.8) | |
| >60 | 185 (21) | 4 (30.8) | |
| Sex | |||
| Male | 607 (69) | 12 (75%) | 0.787 |
| Female | 271 (30.8) | 4 (25%) | |
| Setting | |||
| Rural | 695 (79.15) | 11 (68.7) | 0.350 |
| Urban | 183 (20.8) | 5 (33.3) | |
| Past history of COVID-19 | |||
| Yes | 15 (1.7) | 5 (31.2) | <0.001* |
| No | 863 (98.2) | 11 (68.7) | |
| Comorbidities | |||
| No comorbidities | 627 (71.4) | 3 (18.75) | <0.001* |
| One comorbidities | 164 (18.6) | 4 (25) | |
| Multiple comorbidities | 87 (9.9) | 9 (56) | |
| COVID-19 Vaccination status | |||
| Vaccinated | 9 (1) | 8 (50) | <0.001* |
| Unvaccinated/partially vaccinated | 869 (99) | 8 (50) | |
| ICU admission | |||
| Yes | 285 (32.4) | 3 (18.7) | 0.293 |
| No | 593 (67.5) | 13 (81.3) | |
| Outcome | |||
| Death | 271 (30.8) | 2 (12.5) | 0.169 |
| Recovered | 607 (69.1) | 14 (87.5) |
Clinical profile of admitted patients was distributed based on the degree of severity and outcome. Severity of COVID-19 and age showed a positive correlation with significantly higher severity among those more than 40 years of age. Most of COVID-19 admissions during the Delta wave were in the age group of 41–60 years, out of which 47% of the patients in this age group died and 36.9% were discharged after successful treatment (P < 0.001). In all the categories, males were significantly more affected than females (P < 0.005) including their outcomes (P = 0.013). Most of the patients who did not having any comorbidities remained in the non-severe category, whereas the patients with one or more comorbidities were mostly in severe or critical conditions and found statistically significant including their outcomes (P < 0.001). There was no significant correlation of past history of COVID-19 with disease severity (P = 0.098), while its outcome was statistically significant (P = 0.008) [Tables 2 and 3].
| Indicator | Disease severity during the course of treatment | P-value | ||
|---|---|---|---|---|
| Non-severe n (%) | Severe n (%) | Critical n (%) | ||
| Age group | ||||
| 0–20 | 48 (6.9) | 0 (20) | 3 (1.5) | <0.001* |
| 21–40 | 252 (37.6) | 6 (60) | 32 (16.32) | |
| 41–60 | 205 (37.9) | 32 (20) | 115 (47.9) | |
| >60 | 82 (17.4) | 22 (0) | 81 (34.1) | |
| Sex | ||||
| Male | 424 (71.9) | 36 (60) | 147 (59.6) | 0.005* |
| Female | 153 (28) | 24 (40) | 94 (40.3) | |
| Comorbidities | ||||
| No comorbidities | 482 (83.5) | 26 (43.3) | 18 (7.4) | 0.001* |
| One comorbidity | 84 (14.5) | 23 (38.3) | 159 (65.9) | |
| Multiple comorbidities | 11 (1.9) | 11 (18.3) | 64 (26.5) | |
| Past history of COVID-19 | ||||
| Yes | 13 (1.9) | 1 (20) | 1 (0.5) | 0.098 |
| No | 564 (98) | 59 (80) | 240 (99.5) | |
| Vaccination status | ||||
| Vaccinated | 8 (1.3) | 0 (0) | 1 (0.3) | 0.078* |
| Unvaccinated/partially Vaccinated | 569 (98.6) | 60 (100) | 240 (99.6) | |
| Indicator | Outcome | P-value | |
|---|---|---|---|
| Discharged n (%) | Deceased n (%) | ||
| Age group | |||
| 0–20 | 47 (7.7) | 4 (1.47) | <0.001* |
| 21–40 | 237 (44.9) | 53 (19.5) | |
| 41–60 | 224 (36.9) | 128 (47.2) | |
| >60 | 99 (16.3) | 86 (31.73) | |
| Sex | |||
| Male | 436 (71.8) | 171 (63) | 0.013* |
| Female | 171 (28.2) | 100 (36.9) | |
| Comorbidities | |||
| No comorbidities | 502 (82.7) | 24 (8.8) | 0.001* |
| One comorbidity | 92 (15.1) | 174 (64.2) | |
| Multiple comorbidities | 13 (2.1) | 73 (26.9) | |
| Past history of COVID-19 | |||
| Yes | 15 (2.4) | 0 (0) | 0.008* |
| No | 592 (97.5) | 271 (100) | |
| Vaccination status | |||
| Vaccinated | 8 (1.3) | 1 (0.3) | 0.288 |
| Unvaccinated/partially vaccinated | 599 (98.6) | 270 (99.6) | |
A total of 16 patients found COVID-19 positive were admitted during the Omicron wave, out of which 13 patients were in the non-severe category one patient was severely ill and two patients were in critical condition. All patients with a past history of COVID-19 were in the non-severe category during the Omicron wave and discharged from the hospital after treatment. Patients with one or more comorbidities were found in all non-severe, severe, and critical categories [Tables 4 and 5].
| Indicator | Disease severity during the course of treatment | P-value | ||
|---|---|---|---|---|
| Non-severe n (%) | Severe n (%) | Critical n (%) | ||
| Age group | ||||
| 0–20 | 1 (7.6) | 0 | 0 | 0.751 |
| 21–40 | 4 (30.8) | 0 | 1 (50) | |
| 41–60 | 4 (30.8) | 1 (100) | 1 (50) | |
| >60 | 4 (30.8) | 0 | 0 | |
| Setting | ||||
| Rural | 10 (76.9) | 0 | 1 (50) | 0.231 |
| Urban | 3 (23) | 1 (100) | 1 (50) | |
| Sex | ||||
| Male | 8 (61.5) | 1 (100) | 1 (50) | 0.599 |
| Female | 5 (38.4) | 0 | 1 (50) | |
| Past history of COVID-19 | ||||
| Yes | 5 (38.4) | 0 | 0 | 0.330 |
| No | 8 (61.5) | 1 (100) | 2 (100) | |
| Comorbidities | ||||
| No comorbidities | 3 (23) | 0.449 | ||
| One comorbidities | 4 (30.7) | |||
| Multiple comorbidities | 6 (46.1) | 1 (100) | 2 (100) | |
| Vaccination status | 0.584 | |||
| Vaccinated | 6 (46.1) | 1 (100) | 1 (50) | |
| Unvaccinated/partially vaccinated | 7 (53.8) | 0 | 1 (50) | |
| Indicator | Outcome | P-value | |
|---|---|---|---|
| Discharged n (%) | Deceased n (%) | ||
| Age group | |||
| 0–20 | 1 (7.1) | 0 | 0.712 |
| 21–40 | 5 (35.7) | 1 (50) | |
| 41–60 | 5 (35.7) | 1 (50) | |
| >60 | 3 (21.4) | 0 | |
| Setting | |||
| Rural | 10 (71.4) | 1 (50) | 0.541 |
| Urban | 4 (28.5) | 1 (50) | |
| Sex | |||
| Male | 11 (84.6) | 1 (50) | 0.383 |
| Female | 3 (21.4) | 1 (50) | |
| Past history of COVID-19 | |||
| Yes | 5 (35.7) | 0 | 0.242 |
| No | 9 (64.2) | 2 (100) | |
| Comorbidities | |||
| No comorbidities | 3 (21.4) | ||
| One comorbidities | 4 (28.5) | 0.319 | |
| Multiple comorbidities | 7 (50) | 2 (100) | |
| Vaccination status | |||
| Vaccinated | 8 (57.1) | 0 (0) | 0.893 |
| Unvaccinated/partially vaccinated | 6 (42.8) | 2 (100) |
DISCUSSION
The main objective of this study was to observe the various factors that played role in differences of morbidity and mortality during Delta and Omicron waves in India through the clinical profile of admitted COVID-19-positive patients. In a previous study, it has been observed that during the
Omicron wave, the admitted patients were having less severe illness than in previous waves and fatality was also less as compared to the previous waves.[10]
The first case of Omicron wave in our region was detected on December 26, 2021, then the cases started to rise rapidly and the peak was observed after 4 weeks of the first case and then the third COVID-19 wave declined to almost zero within 10 weeks. A total of 16 admissions were recorded, out of which two (12.5%) deaths occurred, similar admission pattern was observed throughout India including studies worldwide.[5,11-13]
In our study, the mean age of patients during the Delta wave was 46.8 years as compared to 49.25 years during the Omicron wave. The mean age of admitted patients in our study was recorded to be 32.4 and 18.7 years during the Delta and Omicron waves, respectively. These findings are more or less similar to other studies without any significant difference.[12]
During the study period, it was observed that the admission rate of females and males during the Delta wave was 30.8% and 69%, respectively whereas, during the Omicron wave, it was 25% and 75%, respectively. While according to a study the admission rate of females and males during the Delta wave was 54.1% and 45%, respectively, while during the Omicron wave was 56.7% and 43%, respectively.[12] The admission rate depends on various factors influencing the severity of disease condition which in turn depends upon various patient related as well as demographic characteristics of that particular study group.
In our study, we observed 33% of ICU admissions during the Delta wave while 18% of ICU admissions during the Omicron wave. The mortality rate was 30% during the Delta wave, while it was only 12% during the Omicron wave. We also found out that people from rural areas were affected more during both waves. Lower admission rates and mortality were also reported in other studies during the Omicron wave as compared to the Delta wave.[14]
In this study, we observed that 99% of admitted patients during the Delta wave were unvaccinated or partially vaccinated against COVID-19 while during the Omicron wave, 50% of the admitted patients were fully vaccinated with the COVID-19 vaccine. In addition, other studies conducted in the same geographical region reported 98% of the COVID-19 patients who were in home isolation during the Omicron wave and about 65% of the people who were fully vaccinated against COVID-19 did not develop severe symptoms. The reason for a lower number of admissions during the Omicron wave may be attributed to complete vaccination and/or previous exposure to COVID-19.[11] In another study, it was also found that there was a decrease in infection rate in the people who received vaccine against COVID-19.[7]
CONCLUSION
The severity of the disease during the Delta wave was much higher than the Omicron wave. Major contributing factors playing a role in the differences between the Delta wave and Omicron wave may be either complete vaccination status at the time of the Omicron wave or previous exposure due to a history of natural infection with COVID-19 in the past or both. Lack of awareness among the people living in rural areas may be one of the reasons for higher infection rates and transmission during both waves. The previous history of COVID-19 and vaccination drive might be the protective factor against the Omicron variant. The hospital admissions were very low while the degree of severity of the disease as well as the number of deaths were very high during the Delta wave in comparison to the Omicron wave.
Author contributions
Surabhi Shukla: Conceived and designed the analysis, Collected the data, contributed data analysis tools, performed the analysis, wrote the paper. Dr. Peetam Singh: Reviewed the literature, designed the analysis, data analysis, critical review, final approval and editing
Declaration of patient consent
Patient’s consent was not required as patients identity was not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- SARS-CoV-2 omicron variant: Characteristics and prevention. MedComm (2020). 2021;2:838-45.
- [CrossRef] [PubMed] [Google Scholar]
- A focus on the spread of the delta variant of SARS-CoV-2 in India. Indian J Med Res. 2021;153:537-41.
- [CrossRef] [PubMed] [Google Scholar]
- Centers for disease control and prevention 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html [Last accessed on 2023 Feb 03]
- [Google Scholar]
- Investigation of a SARS-CoV-2 B.1.1.529 (Omicron) variant cluster-nebraska, November-December 2021. MMWR Morb Mortal Wkly Rep. 2021;70:1782-4.
- [CrossRef] [PubMed] [Google Scholar]
- Omicron (B.1.1.529 variant of SARS-CoV-2); an emerging threat: Current global scenario. J Med Virol. 2022;94:1780-3.
- [CrossRef] [PubMed] [Google Scholar]
- Probable transmission of SARS-CoV-2 omicron variant in quarantine hotel, Hong Kong, China, November 2021. Emerg Infect Dis. 2022;28:460-2.
- [CrossRef] [PubMed] [Google Scholar]
- Third BNT162b2 vaccination neutralization of SARS-CoV-2 omicron infection. N Engl J Med. 2022;386:492-4.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 incidence and death rates among unvaccinated and fully vaccinated adults with and without booster doses during periods of delta and omicron variant emergence-25 U.S. Jurisdictions, April 4-December 25, 2021. MMWR Morb Mortal Wkly Rep. 2022;2871:132-8.
- [CrossRef] [PubMed] [Google Scholar]
- Genome sequencing reveals a mixed picture of SARS-CoV-2 variant of concern circulation in Eastern Uttar Pradesh, India. Front Med (Lausanne). 2022;8:781287.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical severity of COVID-19 patients admitted to hospitals during the Omicron wave in South Africa: A retrospective observational study. Lancet Glob Health. 2022;10:e961-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of patients infected with delta versus omicron COVID-19 variants presenting to Paris emergency departments: A retrospective cohort study. Ann Intern Med. 2022;175:831-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the clinical features, viral shedding and immune response in vaccine breakthrough infection by the omicron and Delta variants. Research Square 2022 Available from: https://www.researchsquare.com/article/rs-1281925/v1 [Last accessed on 2023 Feb 04]
- [CrossRef] [Google Scholar]
- Increased risk of SARS-CoV-2 reinfection associated with emergence of the omicron variant in South Africa. Science. 2022;376:eabn4947.
- [CrossRef] [PubMed] [Google Scholar]
- Transmissibility, hospitalization, and intensive care admissions due to omicron compared to delta variants of SARS-CoV-2 in Catalona: A cohort study and ecological analysis. Front Public Health. 2022;10:961030.
- [CrossRef] [Google Scholar]




