
Translate this page into:
Assessment of cardiovascular risks, predisposing factors, and awareness of hypertension risk factors among civil servants in Nigeria


*Corresponding author: Unyime Israel Eshiet, Department of Clinical Pharmacy and Biopharmacy, University of Uyo, Uyo, Nigeria. unyimeeshiet@uniuyo.edu.ng
-
Received: ,
Accepted: ,
How to cite this article: Eshiet UI, Orebiyi EP, Umoh IO, Etukudo B, Anwana EE, Gabriel U, et al. Assessment of cardiovascular risks, predisposing factors, and awareness of hypertension risk factors among civil servants in Nigeria. Med India. 2024;3:70-6. doi: 10.25259/MEDINDIA_21_2024
Abstract
Objectives:
The development of hypertension is influenced by a range of factors including diet, obesity, physical activity, family history, and alcohol/tobacco use. This study was aimed at evaluating cardiovascular risks, predisposing risk factors for hypertension, as well as assessing awareness of hypertension and its associated risk factors among civil servants in Akwa Ibom State, Nigeria.
Materials and Methods:
A cross-sectional survey carried out among civil servants working with the Akwa Ibom State Government at the State secretariat in Uyo, Nigeria. A convenient sampling technique was used in recruiting participants for the survey. Recruited participants were interviewed using a suitably designed, pre-tested data collection instrument. The interview was targeted at identifying predisposing risk factors for hypertension among the participants as well as assessing the respondents’ awareness of hypertension and its associated risk factors. Furthermore, the recruited participants were subjected to a cardiovascular risk assessment screening, namely, blood pressure check, pulse rate check, and body mass index determination. Descriptive statistics was used to summarize data, while Pearson’s Chi-square test (χ2) was used to assess the association between variables with statistical significance set at P < 0.05.
Results:
Two hundred and twenty-nine civil servants participated in this study. About 61.6% (141) of the study participants were female, while 129 (56.3%) of the participants had a positive family history of hypertension. About 41.0% (94) of the participants had blood pressure readings in the hypertensive range, with 48 (21.0%) of them being obese. The mean knowledge score of the risk factors for hypertension among the study participants was 5.61 (Standard deviation = ±3.309; Minimum = 0; Maximum = 10), with 36.2% (83) of the participants having a poor level of knowledge (score <5). There was no statistically significant relationship (P > 0.05) between participants’ knowledge of hypertension risk factors and their sociodemographic variables, family history of hypertension, and lifestyle.
Conclusion:
A significant proportion of the participants had a high risk for cardiovascular disorders. The prevalence of predisposing factors for hypertension among the civil servants was high. Knowledge of the risk factors for hypertension was less than optimal. There is a need for enhanced public health enlightenment campaigns on hypertension and its associated cardiovascular risks among this population.
Keywords
Hypertension
Cardiovascular risk
Predisposing factors
Civil servants

INTRODUCTION
Hypertension is often considered a disease of public health importance. It poses a significant threat to the health of adults in sub-Saharan Africa and has been identified as a major contributor to morbidity and mortality in various regions of the world, including sub-Saharan Africa.[1] It has been reported to be a major risk factor for cardiovascular diseases, especially in low-and-middle-income countries such as Nigeria, with a higher prevalence of the disease, poorer control rates, limited awareness, and limited access to treatment when compared with developed regions of the world.[2-4] A previous hypertension prevalence study reported that one in four adult Nigerian is hypertensive.[5] It has also been reported that the unawareness of the disease is a significant cause of cardiovascular events in the Nigeria.[5,6]
Hypertension has often been referred to as a “Silent killer” due to the rare manifestation of symptoms that cause late presentation at healthcare facilities resulting in life-threatening cardiovascular complications.[7] If hypertension is left uncontrolled, it causes heart failure, stroke, myocardial infarction, renal failure, and vision impairment.[8] Although reports from various prevalence studies show a lower prevalence of the condition in young people compared to middle-aged adults and the elderly, pre-hypertension, a precursor for hypertension, has been reported to be more prevalent in young adults, and if detected early, can be treated with lifestyle modification.[9-12] Hence, periodic screening for the early detection and treatment of the disease is of immense importance.[7,13]
Moreover, modification of hypertension-related risk factors is an essential measure in preventing the disease and attaining blood pressure control in persons living with hypertension.[7,14] These risk factors have been broadly categorized as modifiable and unmodifiable risk factors.[12] Modifiable hypertension-related risk factors include physical inactivity, obesity, cigarette smoking, low fruit and vegetable intake, high salt consumption, excess alcohol intake, and a diet high in saturated fat.[7,14,15]
According to a report from a meta-analysis of previous population-based studies published between 1950 and 2013, the estimated prevalence of hypertension in Nigeria, using the diagnostic definition of ≥140/90 mmHg blood pressure reading, is 28.9% (30.6% among the urban population and 26.4% among rural dwellers).[5,16] Studies also suggest that many hypertensive patients are not aware that they are living with the condition.[17,18] This study was aimed at evaluating cardiovascular risks, predisposing risk factors for hypertension as well as assessing awareness of hypertension and its associated risk factors among civil servants in Akwa Ibom State, Nigeria.
MATERIALS AND METHODS
It was a cross-sectional survey carried out among civil servants working with the Akwa Ibom State Government at the State secretariat in Uyo, Nigeria. A convenient sampling technique was used in recruiting participants for the survey. Recruited participants were interviewed using a suitably designed, pre-tested data collection instrument. The interview was targeted at identifying predisposing risk factors for hypertension among the participants as well as assessing the respondents’ awareness of hypertension and its associated risk factors.
Furthermore, the recruited participants were subjected to a cardiovascular risk assessment screening, namely, blood pressure check, pulse rate check, and body mass index determination.
Eligibility criteria
All civil servants employed by the Akwa Ibom Government and working in the State secretariat who provided informed consent to participate in the study were recruited into the study.
Data collection instrument
A suitably designed, pre-piloted, semi-structured, and self-administered questionnaire was used to obtain data from the study participants. The instrument had two sections. The first section was used to obtain data on the sociodemographic details of the respondents and data on lifestyle measures that may be potential risk factors for hypertension among the respondents. The second section comprised questions that assessed the respondents’ knowledge of hypertension and its associated risk factors.
Cardiovascular risk assessment, namely, blood pressure, pulse rate, and body mass index was determined using the Omron blood pressure measuring device for blood pressure/pulse rate determination and a Stadiometer/Weighing scale/Electronic Calculator were used to determine participants body mass index.
Data analysis
Quantitative data were analyzed using Statistical Program and Service Solutions version 25.0 computer package. Descriptive statistics was used to summarize data, while Pearson’s Chi-square test (χ2) was used to assess association between variables with statistical significance set at P < 0.05.
Ethical considerations
Ethical approval for this research work was obtained from the Health Research Ethics Committee of the Akwa Ibom State Ministry of Health (AKSHREC).
RESULTS
Sociodemographic details of study participants
Two hundred and twenty-nine civil servants participated in this study. The majority of the participants (92; 40.2%) were aged between 40 and 49 years, and about 61.6% (141) of the study participants were female. The sociodemographic details of the study participants are presented in Table 1.
| Sn | Parameters | Frequency (n) | Percentage |
|---|---|---|---|
| 1. | Age | ||
| 20–29 | 9 | 3.9 | |
| 30–39 | 45 | 19.7 | |
| 40–49 | 92 | 40.2 | |
| 50–59 | 71 | 31.0 | |
| ≥60 | 12 | 5.2 | |
| 2. | Gender | ||
| Male | 88 | 38.4 | |
| Female | 141 | 61.6 | |
| 3. | Marital status | ||
| Married | 172 | 75.1 | |
| Single | 38 | 16.6 | |
| Divorced/separated | 3 | 1.3 | |
| Widowed | 16 | 7.0 | |
| 4. | Educational level | ||
| Primary | 19 | 8.3 | |
| Secondary | 81 | 35.4 | |
| Tertiary | 129 | 56.3 | |
| 5. | Religion | ||
| Christianity | 229 | 100 | |
| 6. | Tribe | ||
| Ibibio | 146 | 63.8 | |
| Annang | 66 | 28.8 | |
| Oron | 14 | 6.1 | |
| Others | 3 | 1.3 |
Prevalence of predisposing factors to hypertension among study participants
About 23.1% (53) of our study participants reported having a positive family history of hypertension. The proportion of participants who engaged in regular consumption of alcoholic beverages, cigarette smoking, and regular exercises is shown in Table 2.
| Sn. | Factors | Frequency (n) | Percentage |
|---|---|---|---|
| 1. | Family history of hypertension | ||
| Yes | 53 | 23.1 | |
| No | 129 | 56.3 | |
| Do not know | 47 | 20.5 | |
| 2. | Do you consume alcoholic beverages regularly? | ||
| Yes | 90 | 39.3 | |
| No | 139 | 60.7 | |
| 3. | Do you smoke cigarette? | ||
| Yes | 11 | 4.8 | |
| No | 218 | 95.2 | |
| 4. | Do you engage in regular exercises/physical activities? | ||
| Yes | 171 | 74.7 | |
| No | 58 | 25.3 |
Basic cardiovascular parameters of the study participants
About 41% (94) of the participants had blood pressure readings within the hypertensive range. A categorization of the blood pressure, pulse rate, and body mass index of the participants is presented in Table 3.
| Sn. | Parameters | Frequency (n) | Percentage |
|---|---|---|---|
| 1. | Blood pressure (mmHg) | ||
| Within normal range | 135 | 59.0 | |
| Within Grade-1 hypertension range | 60 | 26.2 | |
| Within Grade-2 hypertension range | 34 | 14.8 | |
| 2. | Pulse rate (beats per minute – bpm) | ||
| <60 bpm (Bradycardia) | 5 | 2.2 | |
| 60–100 bpm (normal) | 219 | 95.6 | |
| >100 bpm | 5 | 2.2 | |
| 3. | Body mass index (kg/m2) | ||
| Underweight (<18.5) | 4 | 1.7 | |
| Normal (18.5–<25) | 98 | 42.8 | |
| Overweight (25–<30) | 79 | 34.5 | |
| Obese (≥30) | 48 | 21.0 |
Assessment of blood pressure checks and knowledge of hypertension and its risk factors among the study participants
Results from the assessment of blood pressure checks among the study participants as well as their knowledge of hypertension and its risk factors are presented in Tables 4 and 5, respectively. Furthermore, a categorization of the respondents’ knowledge of the risk factors of hypertension is presented in Figure 1.
| Sn. | Question | Response | |
|---|---|---|---|
| Yes (%) | No (%) | ||
| 1. | Have you ever measured your blood pressure? | 201 (87.8) | 28 (12.2) |
| 2. | Have you ever been diagnosed with hypertension? | 61 (26.6) | 168 (73.4) |
| 3. | Do you know what hypertension is? | 151 (65.9) | 78 (34.1) |
| 4. | Have you ever experienced symptoms that suggest raised blood pressure such as headache and dizziness? | 97 (42.4) | 132 (57.6) |
| 5. | If yes, did you seek medical attention for the symptom (s) | 44 (45.4) | 53 (54.6) |
| 6. | Have you ever received hypertension education from your healthcare provider? | 97 (42.4) | 132 (57.6) |
| Sn | Questions | Responses | ||
|---|---|---|---|---|
| Yes (%) | No (%) | I don’t know (%) | ||
| 1. | Excess salt raises the blood pressure. | 129 (56.3) | 27 (11.8) | 73 (31.9) |
| 2. | Being overweight raises the blood pressure | 140 (61.1) | 24 (10.5) | 65 (28.4) |
| 3. | Regular exercise/physical activities help lower the blood pressure. | 125 (54.6) | 31 (13.5) | 73 (31.9) |
| 4. | Smoking raises the blood pressure | 128 (55.9) | 34 (14.8) | 67 (29.3) |
| 5. | The use of tobacco raises the blood pressure | 118 (51.5) | 29 (12.2) | 83 (36.2) |
| 6. | Regular consumption of alcohol raises the blood pressure. | 122 (53.3) | 27 (11.8) | 80 (34.9) |
| 7. | Regular consumption of fruits and vegetables helps reduce the blood pressure. | 154 (67.2) | 23 (10.0) | 52 (22.7) |
| 8. | High cholesterol levels in the body raises the blood pressure. | 132 (57.6) | 26 (11.4) | 71 (31.0) |
| 9. | Blood pressure increases with age. | 108 (47.2) | 38 (16.6) | 83 (36.2) |
| 10. | Not taking prescribed anti-hypertensive medicines can cause raised blood pressure. | 141 (61.6) | 29 (12.7) | 59 (25.8) |
| Knowledge score | Minimum score: 0.0; Maximum score: 10.0 | |||
| Mean score: 5.61; Standard deviation: ±3.309 | ||||
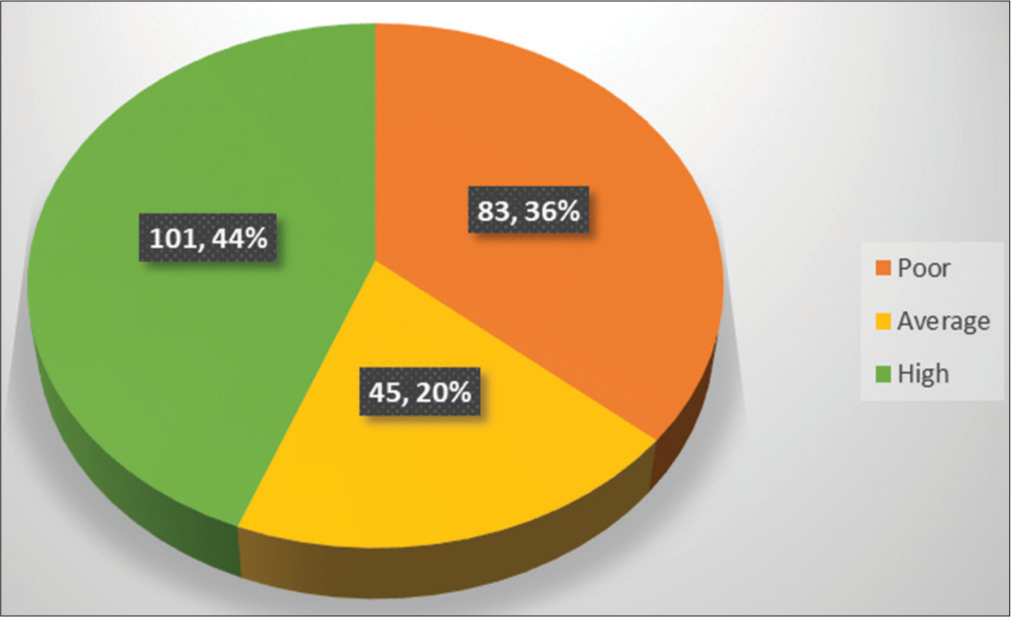
- Categorization of respondents’ level of knowledge of hypertension risk factors.
| Knowledge category | Frequency | Percentage |
|---|---|---|
| Poor (<5) | 83 | 36.2 |
| Average (5–<7) | 45 | 19.7 |
| High (≥7) | 101 | 44.1 |
The mean knowledge score of the risk factors for hypertension among the study participants was 5.61 (Standard deviation = ±3.309; Minimum = 0; Maximum = 10), with 36.2% (83) of the participants having a poor level of knowledge (score <5).
Test of association between respondents’ demographic characteristics and their knowledge of the risk factors for hypertension
We found no statistically significant relationship between the participants’ knowledge the risk factors for hypertension and their sociodemographic parameters, presence of hypertension risk factors, diagnosis of hypertension, and exposure to health education on hypertension [Table 6].
| Sn. | Demographic variable | Pearson Chi-square test | P-value |
|---|---|---|---|
| 1. | Age | 33.205 | 0.768 |
| 2. | Gender | 18.148 | 0.053 |
| 3. | Marital status | 20.793 | 0.894 |
| 4. | Educational level | 30.975 | 0.417 |
| 5. | Tribe | 26.809 | 0.633 |
| 6. | Family history of hypertension. | 19.654 | 0.480 |
| 7. | Alcohol use | 18.072 | 0.583 |
| 8. | Cigarette smoking | 21.295 | 0.360 |
| 9. | Have you ever been diagnosed with hypertension? | 11.528 | 0.318 |
| 10. | Have you ever received hypertension education from your healthcare provider? | 17.294 | 0.634 |
DISCUSSION
Cardiovascular disorders have been reported to be a leading cause of mortality and morbidity in the world including developing countries.[19] The treatment and control of high blood pressure appear to remain inadequate in spite of concerted global clinical and public health interventions.[20] In this study, we evaluated the prevalence of certain cardiovascular risk factors among civil servants working for the Akwa Ibom State government in Nigeria. We found that more than one-third of the study participants had blood pressure readings within the hypertensive range. We also found that more than one-fifth of the civil servants who participated in the study were obese.
Obesity and elevated blood pressure have been identified as major risk factors for cardiovascular disorders. The relationships of these risk factors with cerebrovascular events, peripheral vascular disease, and coronary artery disease are believed to be strong, etiologically significant and predictive.[19] Previous epidemiological studies have established an independent relationship between hypertension and cardiovascular diseases.[15,21] Hypertension continues to pose a major public health threat due to its prevalence and association with cardiovascular morbidity and mortality.[15]
We also assessed exposure to predisposing factors for hypertension among the civil servants. We found that a significant proportion of the study participants had a positive family history of hypertension, consumed alcoholic beverages regularly, engaged in cigarette smoking, and did not engage in regular physical activities. Based on findings from previous epidemiological studies, ethnicity and family history of hypertension are identified as non-modifiable risk factors underlying hypertension.
Family history of hypertension is believed to be among the strongest predictors for developing hypertension as research findings show that individuals with a family history of hypertension are twice as likely to have hypertension as those without a family history of the condition.[15,22] On the other hand, factors such obesity, consumption of alcoholic beverages, cigarette smoking, diet high in saturated fats, and physical inactivity are classified as modifiable risk factors and as such can be reversed.[15,21,23] Thus, a multifactorial approach is required to successfully control blood pressure.
We assessed the knowledge of hypertension and its risk factors among the civil servants. Our results showed that more than one-third of our respondents had a poor knowledge of the condition and its predisposing factors. For instance, less than two-thirds of the respondents were aware of the impact of high salt intake, obesity, physical inactivity, the use of tobacco, regular consumption of alcohol, and inadequate intake of fruits and vegetables on the blood pressure. A study by Gelber et al. found a linear association between higher adiposity measures and the risk of the occurrence of cardiovascular diseases. They reported that higher measures of both overall and central adiposity pose a greater risk of imminent cardiovascular diseases in both men and women, irrespective of the index of measurement.[23] Another study by AlWabel et al.[7] reported a strong association between body mass index and hypertension. They found a higher prevalence of hypertension (34.4%) among obese participants in their study when compared to the prevalence of hypertension (8.6%) among non-obese participants. They also found a positive correlation between the body weight of participants and their average systolic and diastolic blood pressure readings.[7] Reports from other studies have also shown that body mass index is a strong predictor of hypertension.[10,24,25] Although the exact mechanism by which obesity affects blood pressure is not clearly understood, clinical researchers believe that it is due to a combination of elevated leptin levels, insulin resistance, and increased sympathetic activity.[25,26]
A similar study in Seychelles reported that a high proportion of the participants studied demonstrated a good basic knowledge of hypertension. For instance, majority of the respondents were aware of the association of hypertension with salt intake and obesity. Furthermore, majority of the participants recognized cigarette smoking as a risk factor for hypertension and the beneficial effects of physical activity on blood pressure.[27] Another study carried out by Shaikh et al. among entry year students of a medical university in the United Arab Emirates, to identify areas to be emphasized in health promotion practice related to hypertension found that although majority of the participants identified high cholesterol levels, stress, cigarette smoking, high salt intake, and obesity as risk factors of hypertension; majority of the participants were not aware of the association of hypertension with a sedentary lifestyle, the use of oral contraceptives, increasing age, and positive history of cardiovascular diseases and thus did not recognize them as risk factors of hypertension.[28] A similar finding was also reported in a study in Germany where the majority of the participants were not aware of the association between hereditary factors and physical activity with hypertension.[29]
Knowledge of the predisposing risk factors of hypertension among the general population is an essential factor in the modification of lifestyle behaviors among persons toward protecting cardiovascular health.[28] Evaluating the knowledge of modifiable risk factors of hypertension is thus an essential step in identifying misconceptions and knowledge gaps among target populations. Information derived from such assessment would be useful in designing and implementing educational interventions targeted at improving lifestyle behaviors and reducing the incidence and prevalence of hypertension.
More than one-tenth of our respondents reported that they have never checked their blood pressure. We find this a bit disturbing as periodic monitoring of blood pressure is considered an essential clinical investigation in Nigeria and is often offered as a complimentary service, free of charge at several community pharmacies within the country. A similar study among an adult population at Kirtipur municipality in Nepal found that more than one-fifth of the respondents did not check their blood pressure in the past 12 months.[8] They also found that among those that had checked their blood pressure within the past 12 months, the practice of checking blood pressure was more among women than men and also more among those without formal education than those who had formal and higher levels of education. The importance of regular screening for hypertension particularly among adults cannot be overemphasized as the condition is generally asymptomatic and is most often detected during routine blood pressure monitoring. Moreover, the key to preventing the cardiovascular complications of hypertension is early detection of the disease and prompt initiation of clinical interventions.
CONCLUSION
A significant proportion of the participants had a high risk for cardiovascular disorders. The prevalence of risk factors for hypertension among the civil servants was high. Knowledge of the risk factors for hypertension was less than optimal. There is a need for enhanced public health enlightenment campaigns on hypertension and its associated cardiovascular risks among this population.
Limitations
This study was cross-sectional; thus, causation could not be established. Furthermore, some of the data obtained were self-reported; hence, there was a possibility of recall bias.
Author contributions
UE: Conception, study design, data collection, data analysis/interpretation, draft article, and critical review of final manuscript; EO: Conception, study design, data collection, and draft article; IU: Conception, data collection and draft article; BE: Data collection and draft article; EA: Data collection and draft article; UG: Data collection and draft article; ON: Data collection and draft article.
Ethical approval
The research/study approved by the Institutional Review Board at Akwa Ibom State Health Research Ethics Committee, number AKHREC/18/04/23/141, dated May 09, 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate consent from study participants.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- A meta analysis of prevalence rate of hypertension in Nigerian populations. J Public Health Epidemiol. 2011;3:604-7.
- [CrossRef] [Google Scholar]
- Status report on hypertension in Africa-consultative review for the 6th Session of the African Union Conference of Ministers of Health on NCD's. Pan Afr Med J. 2013;16:38.
- [CrossRef] [PubMed] [Google Scholar]
- Global burden of hypertension and systolic blood pressure of at least 110 to 115 mmHg, 1990-2015. JAMA. 2017;317:165-82.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, awareness, treatment, and control of hypertension in Nigeria in 1995 and 2020: A systematic analysis of current evidence. J Clin Hypertens. 2021;23:963-77.
- [CrossRef] [PubMed] [Google Scholar]
- An estimate of the prevalence of hypertension in Nigeria: A systematic review and meta-analysis. J Hypertens. 2015;33:230-42.
- [CrossRef] [PubMed] [Google Scholar]
- Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. World J Cardiol. 2012;4:327-40.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of hypertension and its associated risk factors among medical students in Qassim university. Saudi J Kidney Dis Transpl. 2018;29:1100-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and awareness of hypertension among adults and its related risk factors. J Nepal Health Res Counc. 2017;15:242-6.
- [CrossRef] [PubMed] [Google Scholar]
- Vital signs: Prevalence, treatment, and control of hypertension-United States 1999-2002 and 2005-2008. MMWR Morb Mortal Wkly Rep. 2011;60:103-8.
- [Google Scholar]
- Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: A national survey. Int J Hypertens. 2014;2014:564679.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertension in young adults-An under-estimated problem. Singapore Med J. 2003;44:448-52.
- [Google Scholar]
- The prevalence of hypertension and its modifiable risk factors among medical students of a medical college in Uttar Pradesh, India. J Lumbini Med Coll. 2013;1:53-5.
- [Google Scholar]
- The association between risk factors and hypertension in Perak, Malaysia. Med J Malaysia. 2013;68:291-6.
- [Google Scholar]
- Prevalence of hypertension and blood pressure profile amongst urban-dwelling adults in Nigeria: A comparative analysis based on recent guideline recommendations. Clin Hypertens. 2019;25:7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of hypertension, obesity, diabetes, and metabolic syndrome in Nepal. Int J Hypertens. 2011;2011:821971.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and associated risk factors of hypertension among people aged 50 years and more in Banepa Municipality, Nepal. Kathmandu Univ Med J. 2012;10:35-8.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of cardiovascular risk factors among university students: The gender factor. Cardiol Res. 2012;3:172-9.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge of risk factors for hypertension in a rural Indian population. Heart Asia. 2019;11:e011136.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, awareness, treatment and control of hypertension in Malaysia: A national study of 16,440 subjects. Public Health. 2008;122:11-8.
- [CrossRef] [PubMed] [Google Scholar]
- Are there interactions and relations between genetic and environmental factors predisposing to high blood pressure? Hypertension. 1991;18(3 Suppl):I29-37.
- [CrossRef] [Google Scholar]
- Measures of obesity and cardiovascular risk among men and women. J Am Coll Cardiol. 2008;52:605-15.
- [CrossRef] [PubMed] [Google Scholar]
- Overweight and obesity in relation to cardiovascular disease risk factors among medical students in Crete, Greece. BMC Public Health. 2003;3:3.
- [CrossRef] [PubMed] [Google Scholar]
- Role of sympathetic nervous system and neuropeptides in obesity hypertension. Braz J Med Biol Res. 2000;33:605-18.
- [CrossRef] [PubMed] [Google Scholar]
- Weight gain-induced blood pressure elevation. Hypertension. 2000;35:1135-40.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, attitudes, and practices on hypertension in a country in epidemiological transition. Hypertension. 1998;31:1136-45.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge regarding risk factors of hypertension among entry year students of a medical university. J Family Community Med. 2011;18:124-9.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge and attitudes towards hypertension and hypercholesterolemia in a population of Southern Germany: Results from a population survey in the Augsburg area. Soz Praventivmed. 1991;36:5-8.
- [CrossRef] [PubMed] [Google Scholar]




