
Translate this page into:
Echocardiographic assessment of patients with end-stage renal disease undergoing maintenance hemodialysis


*Corresponding author: Roshan Bhandari, Department of Internal Medicine, Institute of Medicine, Tribhuvan University Teaching Hospital, Kathmandu, Nepal. bhandariroshan369@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhandari R, Pantha S, Pandey G, Paudyal R. Echocardiographic assessment of patients with end-stage renal disease undergoing maintenance hemodialysis. Med India 2023;2:15.
Abstract
Objectives:
Chronic kidney disease is a global health problem. End-stage renal disease (ESRD) patients have a high frequency of cardiac functional and structural abnormalities associated with higher mortality. Echocardiography is a valuable tool to assess cardiac structural and functional changes, which helps in stratifying prognostic risk factors and measuring the effectiveness of therapeutic intervention.
Materials and Methods:
We conducted a prospective, cross-sectional, hospital-based study for 1 year from 2076/11/05 to 2077/11/05 B.S (February 17, 2020, to February 17, 2021, A.D. Total of 65 patients with the diagnosis of ESRD undergoing maintenance hemodialysis (MHD) at Chitwan Medical College Hospital meeting inclusion criteria were enrolled. Detailed history, examinations, echocardiographic, and laboratory findings were recorded, and their association was compared with different explanatory variables. Data were analyzed using Statistical Package for the Social Sciences version 25.
Results:
The most common echocardiography finding among the 65 patients was valvular heart disease (VHD) (78.50%). Among them, 86.2% were undergoing hemodialysis (HD) twice weekly. About 92.7% had hypertension and 52.3% had diabetes mellitus. All had anemia with a mean hemoglobin of 7.86 ± 1.30 g/dL. The most common echocardiography finding was VHD (78.50%). There were statistically significant associations between the age of patients with a prevalence of VHD and systolic dysfunction; the presence of global hypokinesia with body mass index; and the presence of left ventricular hypertrophy (LVH) with calcium levels. Furthermore, a statistically significant difference in the duration of HD was observed with LVH.
Conclusion:
Cardiovascular diseases are the major cause of morbidity and mortality among ESRD patients undergoing MHD. The study identifies various factors influencing echocardiographic parameters in ESRD patients and highlights VHD as the most prevalent echocardiographic finding. It also emphasizes the importance of echocardiography as a valuable tool for assessing cardiac changes in these patients, aiding in risk stratification and the evaluation of therapeutic interventions.
Keywords
Chronic kidney disease
Echocardiography
End-stage renal disease
Hemodialysis
Valvular heart disease

INTRODUCTION
The worldwide estimated prevalence of chronic kidney disease (CKD) is 13.4% (11.7–15.1%) and patients with end-stage renal disease (ESRD) needing renal replacement therapy is estimated between 4.902 and 7.083 million.[1,2] Cardiovascular disease (CVD) is the major cause of morbidity and mortality in patients with CKD. Coronary artery disease including myocardial infarction, congestive heart failure, and pericardial disease is the common manifestation of CKD. Heart failure accounts for 15%, myocardial infarction about 10%, and pericarditis about 3% of dialysis-associated mortality.[3,4]
MATERIALS AND METHODS
It was a quantitative, prospective, and cross-sectional hospital-based study. The study was conducted in the Department of Internal Medicine (Nephrology), Chitwan Medical College and Teaching Hospital (CMCTH), Bharatpur, Nepal, from 2076/11/05 to 2077/11/05 B.S (February 17, 2020, to February 17, 2021, A.D). Ethical clearance was taken before initiation of the study according to the norms of the Institutional Review Committee (CMC-IRC). Consent was obtained from all the patients enrolled in the study. Inclusion criteria: (1) Age ≥18 years and (2) patients with ESRD undergoing maintenance hemodialysis (MHD) for more than 3 months. Exclusion criteria: (1) Patients who were diagnosed with cardiac disease, rheumatic heart disease, myocarditis, and primary heart muscle disease like cardiomyopathies before initiation of hemodialysis (HD); (2) patients who did not give written consent; and (3) patients who were critically ill required intensive care unit care during the study period.
A total of 65 cases fulfilling the inclusion and exclusion criteria were included in the study.
Sample Size (N) = Z2 p (1–p)/C2
Z = 1.96, Z = constant C = 10 % confidence interval
P = 20% P = Prevalence of CVD in patients with renal impairment (In a study of 6,223 people in the Framingham study, 18% of men and 20% of women with renal impairment had CVD).
Detailed clinical history of the patients was collected, and relevant clinical examination of all participants was done by the researcher himself. Confidentiality of the information of the respondents was maintained. Two-dimensional transthoracic echocardiography was done by a qualified cardiologist using the echocardiogram (model: Siemens acusonx 700) in the Department of Cardiology, CMCTH.
Left ventricular hypertrophy (LVH): The cutoff value of LVH is >115 g/m2 for men and >95 g/m2 for women.[5] In cases of HD patients, there are large bodyweight variations, which may lead to evaluation errors by body surface indexation. Thus, to calculate left ventricular (LV) mass accurately in HD patients some experts recommended indexing LV mass by height to the 2.7 power.[6]
LV systolic dysfunction: LV systolic dysfunction is assessed by measuring ejection fraction (EF) and fractional shortening by echocardiography. EF is calculated by following the formula:
EF = (LVEDV-LVESV)/LVEDV
where,
LVEDV=Left Ventricular End Diastolic Volume
LVESV=Left Ventricular End Systolic Volume
LV EFs of <52% and <54% for men and women, respectively, are indicative of abnormal LV systolic function.[5]
c) LV diastolic dysfunction: Diastolic dysfunction is characterized by alterations in ventricular relaxation and compliance. Subsequently, it is frequently followed by a compensatory increase in filling pressure in more advanced stages.[7]
Diastolic function was assessed using several parameters including the pattern of mitral inflow and the ratio of peak early (E) filling velocity to late diastolic filling (A) velocity (E/A ratio), deceleration time of early filling velocity (DT), and the isovolumic relaxation time.[8]
Normal serum sodium concentration in our body is 135–145 Mm. it is defined as hyponatremia when its concentration is below 135 Mm and more than 145 Mm is leveled as hypernatremia.[9]
Normal serum potassium concentration in our body is 3.5 mm to 5.5 mm. It is defined as hypokalemia when its concentration is below 3.5 mm and more than 5.5 mm is leveled as hyperkalemia.[10]
Normal serum calcium is approximately 8.6–10.2 mg/dL below 8.6 mg/dL it is considered hypocalcemia and above 10.2 it is leveled as hypercalcemia.
Body mass index (BMI) = Body weight (kilograms) divided by height squared (meters) According to the World Health Organization (WHO);[11]
Underweight BMI in the range of 15–19.9 kg/m2
Normal weight if the BMI is 20–24.9 kg/m2
Overweight if the BMI is 25–29.9 kg/m2
Obese if it is 30–35 kg/m2 or greater.[11]
The WHO criteria for anemia in men is <13 g/dL in men and <12 g/dL in women. However, it differs by age, sex, and pregnancy status.[12]
Data were collected using a self-designed structured pro forma. The collected data were checked, reviewed, and organized for accuracy. The data were entered and analyzed using the Statistical Package for the Social Sciences (IBM SPSS) version 20. Data were summarized using descriptive statistics (frequency, percentage, central tendency, and dispersion). The Chi-square test or Fisher exact test at a 5% level of significance was used to determine the association between variables.
Patients with CKD having CVD had a 3–30 times higher risk of mortality as compared to the general population.[3] Evaluation of echocardiographic parameters in patients with CKD can provide invaluable information regarding the disease.[4]
The objectives of the study include echocardiographic assessment among ESRD patients undergoing (MHD); to identify the magnitude of systolic and diastolic dysfunction, LVH, regional wall motion abnormality, pericardial effusion and valvular heart disease (VHD); and the association between the findings with laboratory parameters and some explanatory variables.
RESULTS
A total of 65 patients were enrolled during the study period over 1 year, among which 50% were male and 45.50% were female [Figure 1]. The most common echocardiography finding [Figure 2] in our study was VHD (78.50%), of which the most common VHD [Figure 3] was mitral regurgitation (64.61%) and the least prevalent abnormality was pulmonary regurgitation (1.50%). The prevalence of other findings [Figure 2] in descending order was LV diastolic dysfunction (72.30%), LVH (60%), LV systolic dysfunction (27.70%), pericardial effusion (18.50%), and global hypokinesia (12.30%). The most common frequency of HD [Table 1] was twice a week (86.2%). The most common religion among the patients was Hinduism (95.4%). The mean height was 63.31 inches (standard deviation [SD] 2.474 range 57–72) and the weight was 53.98 kg (SD 10.43 range 30.53–81.72). Overall, 52.3% had a history of diabetes, 92.7% had hypertension, 46.2% had a smoking habit, and 43.1 % had a drinking alcohol habit [Table 1]. The mean hemoglobin was 7.86 ± 1.30 in which the maximum hemoglobin was 10.8 and the minimum was 4.3. It appeared that most of the people had normal serum potassium (53.80%), normal serum Sodium (72.30%), and normal serum calcium (60%); however, there were no cases of hypercalcemia [Figure 4]. The results of bivariate analyses between Echocardiography findings and different independent variables among ESRD patients are shown in [Tables 2 and 3], and the correlation between echocardiography variables with duration in ESRD on HD is shown in [Table 4].
| Variables | Category | Frequency (%) |
|---|---|---|
| Diabetes mellitus | ||
| Presence | 34 (52.3) | |
| Absence | 31 (47.7) | |
| Hypertension | ||
| Presence | 60 (92.3) | |
| Absence | 5 (7.7) | |
| Smoking habit | ||
| Yes | 30 (46.2) | |
| No | 35 (53.8) | |
| Alcohol habit | ||
| Yes | 28 (43.1) | |
| No | 37 (56.9) | |
| Duration of hemodialysis | ||
| <1 year | 18 (27.6) | |
| >1 years | 47 (72.4) | |
| Frequency of hemodialysis | ||
| Once a week | 8 (12.3) | |
| Twice a week | 56 (86.2) | |
| Thrice a week | 1 (1.5) |
ESRD: End-stage renal disease, CMCTH: Chitwan medical college and teaching hospital
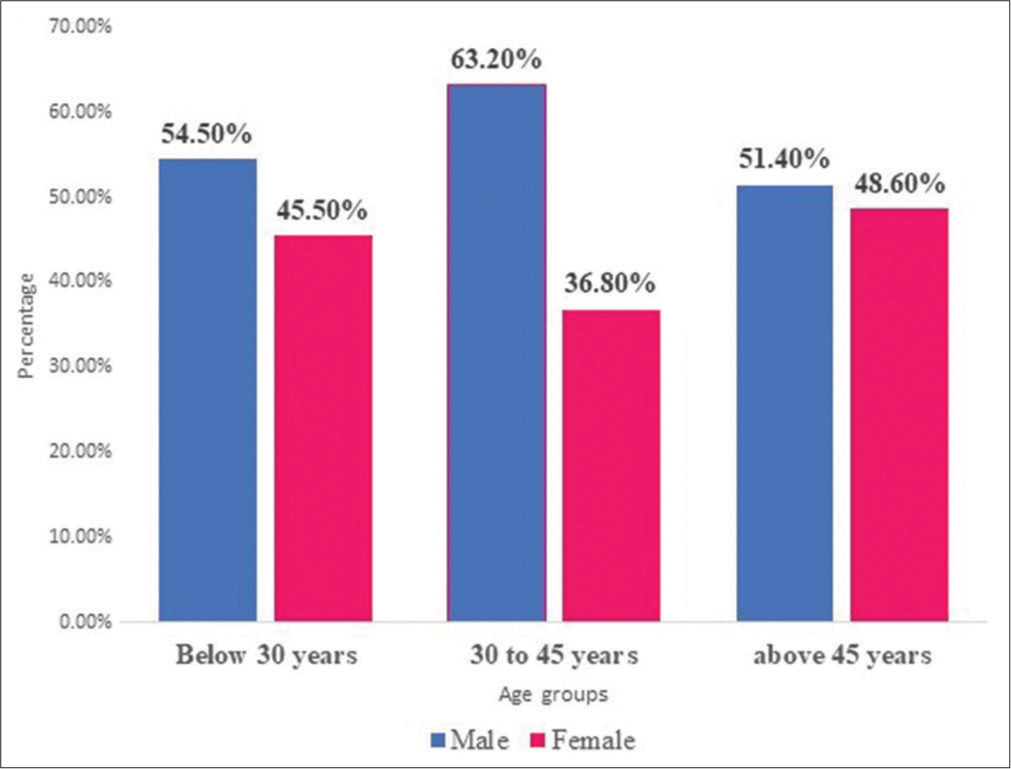
- Age-sex distribution among end-stage renal disease patients undergoing maintenance hemodialysis attending Chitwan Medical College and Teaching Hospital.

- Echocardiographic findings among end-stage renal disease patients undergoing maintenance hemodialysis attending Chitwan Medical College and Teaching Hospital.
| Variables | Valvular heart disease | Global hypokinesia | Pericardial effusion |
|---|---|---|---|
| Frequency (%) | Frequency (%) | Frequency (%) | |
| Age group | |||
| 45 and below | 27 (90) | 3 (37.5) | 6 (20) |
| Above 45 | 24 (68.6) | 5 (62.5) | 6 (17.1) |
| Sex | |||
| Male | 31 (86.1) | 6 (75) | 7 (19.4) |
| Female | 20 (69) | 2 (25) | 5 (17.2) |
| BMI | |||
| Normal | 28 (71.8) | 3 (37.5) | 5 (12.8) |
| Others | 23 (88.5) | 5 (62.5) | 7 (26.9) |
| HTN | |||
| Presence | 46 (76.7) | 8 (100) | 11 (18.3) |
| Absence | 5 (100) | 0 | 1 (20) |
| DM | |||
| Presence | 25 (73.5) | 4 (50) | 6 (17.6) |
| Absence | 26 (83.9) | 4 (50) | 6 (19.4) |
| Smoking | |||
| Yes | 24 (80) | 4 (50) | 4 (13.3) |
| No | 27 (77.1) | 4 (50) | 8 (22.9) |
| Alcohol | |||
| Yes | 23 (82.1) | 4 (50) | 4 (14.3) |
| No | 28 (75.7) | 4 (50) | 8 (21.6) |
| Potassium level | |||
| Normal | 29 (82.9) | 4 (50) | 7 (20) |
| Hypokalemia/Hyperkalemia | 22 (73.3) | 4 (50) | 5 (16.7) |
| Sodium level | |||
| Normal | 36 (76.6) | 5 (62.5) | 7 (14.9) |
| Hyponatremia/Hypernatremia | 15 (83.3) | 3 (37.5) | 5 (27.8) |
| Calcium Level | |||
| Normal | 20 (76.9 | 4 (50) | 4 (15.4) |
| Hypocalcemia/Hypercalcemia | 31 (79.5) | 4 (50) | 8 (20.5) |
ESRD: End-stage renal disease, BMI: Body mass index, HTN: Hypertension, DM: Diabetes mellitus
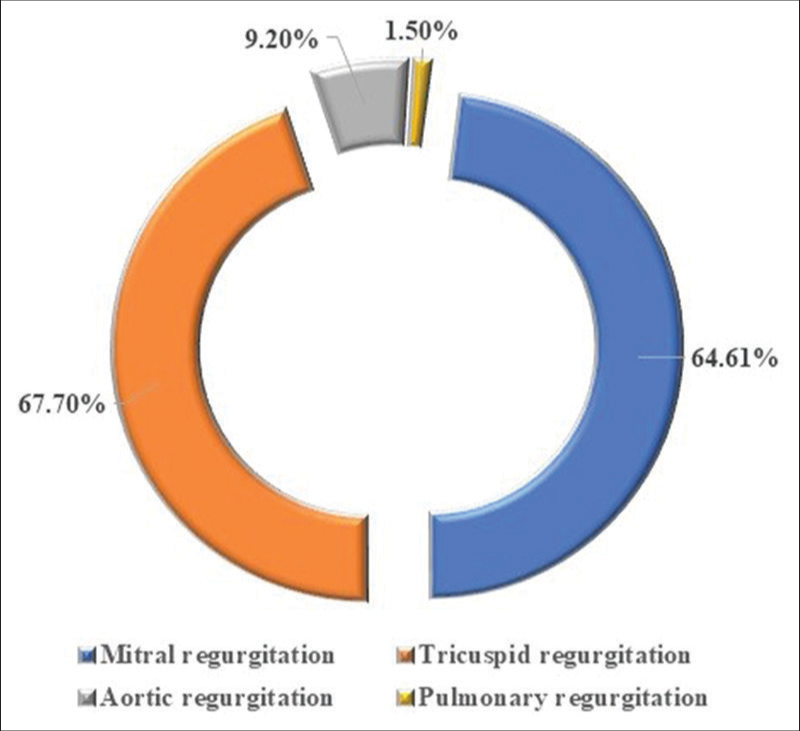
- Valvular heart disease among end-stage renal disease patients undergoing maintenance hemodialysis attending Chitwan Medical College and Teaching Hospital.
| Variables | Left ventricular hypertrophy | Systolic dysfunction | Diastolic dysfunction |
|---|---|---|---|
| Frequency (%) | Frequency (%) | Frequency (%) | |
| Age group | |||
| Below 45 | 17 (56.7) | 12 (40) | 19 (63.3) |
| 45 above | 22 (62.9) | 6 (17.1) | 28 (80) |
| Sex | |||
| Male | 22 (61.1) | 12 (33.3) | 25 (69.4) |
| Female | 17 (58.6) | 6 (20.7) | 22 (75.9) |
| BMI | |||
| Normal | 23 (59) | 10 (25.6) | 31 (79.5) |
| Others | 16 (61.5) | 8 (30.8) | 16 (61.5) |
| HTN | |||
| Presence | 36 (60) | 17 (28.3) | 43 (71.7) |
| Absence | 3 (60) | 1 (20) | 4 (80) |
| DM | |||
| Presence | 20 (58.8) | 10 (29.4) | 26 (76.5) |
| Absence | 19 (61.3) | 8 (25.8) | 21 (67.7) |
| Smoking | |||
| Yes | 20 (66.7) | 10 (33.3) | 24 (80) |
| No | 19 (54.3) | 8 (22.9) | 23 (65.7) |
| Alcohol | |||
| Yes | 16 (57.1) | 9 (32.1) | 21 (75) |
| No | 23 (62.2) | 9 (24.3) | 26 (70.3) |
| Potassium level | |||
| Normal | 21 (60) | 9 (25.7) | 26 (74.3) |
| Hypokalemia/hyperkalemia | 18 (60) | 9 (30) | 21 (70) |
| Sodium level | |||
| Normal | 31 (66) | 14 (29.8) | 37 (78.7) |
| Hyponatremia/hypernatremia | 8 (44) | 4 (22.2) | 10 (55.6) |
| Calcium | |||
| Normal | 12 (46.2) | 8 (30.8) | 15 (57.7) |
| Hypocalcemia/hypercalcemia | 27 (69.2) | 10 (25.6) | 32 (82.1) |
ESRD: End-stage renal disease, BMI: Body mass index, HTN: Hypertension, DM: Diabetes mellitus

- Distribution of potassium, sodium, and calcium levels among end-stage renal disease patients undergoing maintenance hemodialysis attending Chitwan Medical College and Teaching Hospital.
| Echocardiographic findings | Duration | |
|---|---|---|
| ≤12 months | >12 months | |
| Left ventricular hypertrophy | ||
| Yes | 1 | 39 |
| No | 17 | 8 |
| Left ventricular diastolic dysfunction | ||
| Yes | 4 | 43 |
| No | 4 | 14 |
| Valvular heart disease | ||
| Yes | 7 | 44 |
| No | 1 | 13 |
| Left ventricular systolic dysfunction | ||
| Yes | 0 | 18 |
| No | 8 | 39 |
| Mitral regurgitation | ||
| Yes | 1 | 41 |
| No | 17 | 6 |
| Pericardial effusion | ||
| Yes | 3 | 9 |
| No | 5 | 48 |
| Global Hypokinesia | ||
| Yes | 0 | 8 |
| No | 8 | 44 |
ESRD: End stage renal disease
DISCUSSION
In our study, 50% were males and 45.50% were females, males were predominant which was found to be similar in other studies.[13,14] The average age of our study population was 47.45 years. This was nearly the same in many other studies.[15,16] The maximum number of patients undergoing HD in our hospital were from Bharatpur Metropolitan City (35.4%) and Kawasoti (4.1%). The majority of them were Hindu (95.4%) by religion.[17] These demographic factors may vary based on locality, culture, and religion. Hypertension (92.30%) was by far the most prevalent comorbidity observed in ESRD patients in our study. Hypertension is related to both a cause and effect in CKD patients, controlling hypertension not only slows the progression of renal damage but also reduces the risk of CKD.[18] A study done in the USA estimated that hypertension occurs in 35.8% of stage 1, 48.1% of stage 2, 59.9% of stage 3, and 84.1% of stage 4–5 CKD patients.[19]
The majority of patients in our study were undergoing HD twice a week (86.2%), followed by thrice a week (1.5%) and once a week (12.3%) for 4 h per session. The mean hemoglobin level in our study was 7.86 ± 1.30 g/dL and 100% had anemia (hemoglobin [Hb] <11 g/dL). A study by Adera et al. shows that the prevalence of anemia increased with worsening kidney function: stage 1 and 2, 3A, 3B, 4, and 5 CKD were 20%, 44.8%, 46.4%, 81.1%, and 93.8%, respectively. Severe anemia (Hb <8 g/ dL) was documented in 49/251 (19.5%) of CKD patients.[20] The average level of serum calcium and serum phosphorus was 7.91 mg/dL, and 4.97 ± 1.34 mg/dL, respectively, in our study. The mean level of Hb, serum calcium, serum phosphorus, and serum albumin observed in the study by Hamin et al. was 10.98 + 1.4 g/dL, 281.5 pg/mL, 0.75 ±1.34 mg/dL, and 3.66 ± 0.39 g/dL, respectively.[21]
The most common echocardiography finding in our study was VHD which was seen in 51 patients (78.52%). The other findings in descending order were LV diastolic dysfunction (LVDD) (72.30%), LVH (60%), LV systolic dysfunction (27.70%), pericardial effusion (18.5%), Global hypokinesia (12.3%), and regional wall motion abnormalities nil. The major echocardiographic changes observed by Saxena et al. was VHD: tricuspid regurgitation (TR) in 33(66%) mitral regurgitation (MR) in 24 (48%) patients LVH in 29 (58%) patients, LVDD in 25 (50%) patients, pericardial effusion in 10 (20%) patients, pulmonary hypertension in 23 (46%) patients, dilated left atrium in 14 (28%) patients, dilated left ventricle in 4 (8%) patients, and regional wall motion abnormalities in 3 (6%) patients also there was no cases of valvular calcification.[22] There was a statistically significant association between age group and prevalence of VHD in our study which was similar to different another study. Data from the US Renal Data System in 2017 showed that the prevalence of VHD diagnoses was 14% among patients with CKD compared with 7% in the medicare survey of patients aged >65.[23] Furthermore, the presence of LVH was found to be significantly associated with the serum calcium level. A study by Nitta et al. also shows a significant association with hypocalcemia although the mechanism is not completely known, hypocalcemia followed by Vitamin D deficiency may be associated with the pathogenesis of LVH.[24]
The presence of global hypokinesia was also found to be statistically significant with the BMI. In our study 39 patients had normal BMI, eight patients had overweight, and 18 patients were underweight. Malnutrition increases the risk of morbidity and mortality among ESRD patients undergoing HD. Being overweight is one of the risk factors for hypertension and diabetes mellitus which are the most common etiological factors of ESRD. The presence of systolic dysfunction was found to be statistically significant with the age of the patient in our study which was not found to be significant in other similar studies.
The duration of HD also plays an important role in cardiovascular outcomes.[25] In our study, HD duration was categorized into ≤12 months and >12 months. Thirty-nine patients who were doing HD for >12 months developed LVH compared to 1 patient in the ≤12 months group. Our study showed a significant correlation between longer duration of HD and LVH (P < 0.0001). In the study by Kaze et al. also observed a significant positive relation between longer duration of HD and LVH (P < 0.047).[26] LVH is reported in 16–50% of early and intermediate CKD (Stages 1–3) patients, 50–70% of advanced CKD (Stages 4 and 5) patients, and in up to 70–90% of regular dialysis patients.[27]
Another echocardiography parameter that was found to be statistically correlated with the duration of HD in our study was MR (P < 0.0001). These results were in contrast to many other studies.[28]
CONCLUSION
The study holds significant clinical importance as it addresses the escalating global issue of CKD. HD remains the predominant renal replacement therapy for sustaining patients. CVDs contribute significantly to morbidity and mortality in ESRD patients undergoing HD. The study identifies various factors influencing echocardiographic parameters in these patients and highlights VHD as a prevalent echocardiographic finding. Significantly, echocardiography emerges as the simplest yet most reliable method for evaluating cardiac function in ESRD patients on HD. This emphasizes the crucial role of echocardiography in detecting cardiac abnormalities, thus aiding in risk assessment and guiding appropriate interventions for these patients.
Authors contributions
Roshan Bhandari: Concept, design, literature search, manuscript preparation, statistical analysis and editing, data analysis. Srijan Panth: Concept, design, literature search, manuscript preparation, data acquisition and analysis. Ghanashyam Pandey: Concept, design, literature search, manuscript preparation, statistical analysis and editing. Richa Paudyal: Concept, design, literature search, manuscript preparation, statistical analysis and editing. Guarantors: Roshan Bhandari, Srijan Pantha.
Declaration of patient consent
Institutional Review Board (IRB) permission was obtained for the study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011;80:17-28.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and disease burden of chronic kidney disease. Adv Exp Med Biol. 2019;1165:3-15.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular risk factors in CKD associate with both ESRD and mortality. J Am Soc Nephrol. 2013;24:1159-65.
- [CrossRef] [PubMed] [Google Scholar]
- Echocardiographic changes in chronic kidney disease patients on maintenance hemodialysis. Cureus. 2020;12:e8969.
- [CrossRef] [Google Scholar]
- Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28:1-39.e14.
- [CrossRef] [PubMed] [Google Scholar]
- Echocardiography in chronic kidney disease: Diagnostic and prognostic implications. Nephron Clin Pract. 2010;114:c242-7.
- [CrossRef] [PubMed] [Google Scholar]
- Current perspectives in diastolic dysfunction and diastolic heart failure. Heart. 2006;92:712-8.
- [CrossRef] [PubMed] [Google Scholar]
- Canadian randomized trial of hemoglobin maintenance to prevent or delay left ventricular mass growth in patients with CKD. Am J Kidney Dis. 2005;46:799-811.
- [CrossRef] [PubMed] [Google Scholar]
- Harrison's Principles of Internal Medicine (20th ed). United States: McGraw Hill; 2018.
- [Google Scholar]
- Body mass index: Obesity, BMI, and health: A critical review. Nutr Today. 2015;50:117-28.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical evaluation of different types of anemia. World J Anemia. 2018;2:26-30.
- [CrossRef] [Google Scholar]
- Clinical and etiological profile of chronic kidney disease patients on hemodialysis in a tertiary care hospital in Northern part of Bangladesh. IOSR J Dent Med Sci. 2018;17:42-5.
- [Google Scholar]
- Clinical and epidemiological profile of chronic kidney disease patients in a tertiary care referral centre in South India. Int J Community Med Public Health. 2016;3:3487-92.
- [CrossRef] [Google Scholar]
- Practice pattern of hemodialysis among end-stage renal disease patients in rural South India: A single-center experience. Saudi J Kidney Dis Transpl. 2017;28:1150-6.
- [CrossRef] [PubMed] [Google Scholar]
- Hemodialysis outcomes and practice patterns in end-stage renal disease: Experience from a Tertiary care hospital in Kerala. Indian J Nephrol. 2017;27:51-7.
- [CrossRef] [PubMed] [Google Scholar]
- Religion and conservation: A review of use and protection of sacred plants and animals in Nepal. J Inst Sci Technol. 2015;20:61-6.
- [CrossRef] [Google Scholar]
- Management of hypertension in chronic kidney disease. Drugs. 2019;79:365-79.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertension in chronic kidney disease: Navigating the evidence. Int J Hypertens. 2011;2011:132405.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of anemia and its associated factors among chronic kidney disease patients at university of Gondar hospital, Northwest Ethiopia: A hospital-based cross sectional study. Int J Nephrol Renovasc Dis. 2019;12:219-28.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical characteristics of patients on long-term hemodialysis. J Coll Physicians Surg Pak. 2019;29:328-32.
- [CrossRef] [PubMed] [Google Scholar]
- Case series role of 2-D echocardiography in detecting cardiovascular abnormalities in chronic kidney disease patients: Case series of 50 chronic kidney disease patients. IAIM. 2017;4:122-6.
- [Google Scholar]
- Chronic kidney disease and valvular heart disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;96:836-49.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for increased left ventricular hypertrophy in patients with chronic kidney disease: Findings from the CKDJAC study. Clin Exp Nephrol. 2019;23:85-98.
- [CrossRef] [Google Scholar]
- Echocardiographic profile in patients under maintenance haemodialysis. IOSR J Pharm. 2015;5:35-7.
- [Google Scholar]
- Pattern and correlates of cardiac lesions in a group of sub-Saharan African patients on maintenance hemodialysis. Pan Afr Med J. 2014;17:3.
- [CrossRef] [PubMed] [Google Scholar]
- The role of echocardiographic study in patients with chronic kidney disease. J Formos Med Assoc. 2015;114:797-805.
- [CrossRef] [PubMed] [Google Scholar]
- Association of serum phosphorus, calcium and parathyroid hormone with cardiovascular calcification in regular hemodialysis patients. J Parathyr Dis. 2017;6:44-9.
- [CrossRef] [Google Scholar]




