
Translate this page into:
Meningioma: Is apparent diffusion coefficient value of any importance? A study from the tertiary care center
 , Rakesh Kumar6
, Rakesh Kumar6

*Corresponding author: Saurabh Maheshwari, Department of Radiodiagnosis and Imaging, Military Hospital Shimla, Shimla, Himachal Pradesh, India. saurabhmhshwr@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Sahu S, Maheshwari S, Bhattacharjee S, Maria V, Mendiratta P, Kumar R. Meningioma: Is apparent diffusion coefficient Value of any importance? A study from the tertiary care center. Med India 2022;1:15.
Abstract
Objectives:
Meningiomas are one of the most common intracranial tumors accounting for 14–20% of all intracranial tumors. Diffusion-weighted imaging (DWI) along with the calculation of apparent diffusion coefficient (ADC) is a novel, non-invasive, and reliable technique of choice for the pre-operative assessment and the treatment planning of different types of meningiomas. Our study aimed to correlate the ADC values of meningiomas with their histopathological grade.
Materials and Methods:
We studied 21 patients with meningioma. These were initially diagnosed on imaging and confirmed on histopathology. We calculated the normalized ADC (NADC) values from the DWI of their lesion. NADC values and atypical morphological features were utilized to type the meningiomas as typical or atypical. These findings were correlated with histopathological reports of grading of meningioma.
Results:
There was no significant correlation between the grades of meningioma and the ADC values. The normalized ADC values varied from 0.14 to 1.37 × 10−3 mm2/s for Gr I meningioma in our series and most of our cases fell in this category of meningioma. We had a solitary case of Gr-II meningioma and the ADC value for this lesion was 1.26 × 10−3 mm2/s.
Conclusion:
Meningiomas are a common group of tumors in the brain with a quest to characterize the grades preoperatively on imaging. The NADC is a better method as compared to plain ADC values for this purpose. In our series, we did not find any correlation of NADC on pre-operative imaging to the grades of tumors.
Keywords
Meningioma
Diffusion-weighted imaging
Apparent diffusion coefficient
Normalized ADC
Magnetic resonance imaging

INTRODUCTION
Meningiomas account for 14–20% of all intracranial tumors. They are graded as benign (Gr I), atypical (Gr II), and malignant (Grade III) as per the WHO 2016 classification. Among these, there are 10% of cases are either atypical or malignant.[1] On imaging itself, typical meningiomas are easy to identify, while atypical meningiomas have some features to suggest atypical features on imaging. These are edema, mass effect, heterogeneous post-contrast enhancement, and irregular cerebral surfaces. However, these markers cannot be utilized as definitive markers for differentiating benign from the malignant lesion.[2] Hence, there is an eternal search for a diagnostic method or criteria for accurate differentiation between benign and malignant meningiomas before surgery, to aid in surgical and treatment planning.
Diffusion-weighted imaging (DWI) is a recent, non-invasive technique for the imaging of brain tumors.[3] It also assists in therapeutic planning. There have been numerous attempts to test the usefulness of DWI in grading meningiomas, with variable degrees of success.[4]
The objective of our study was to evaluate the value of DWI in grading meningiomas according to the severity and then search for a correlation with the histopathological report. A pre-operative characterization of disease would be of great importance for treatment planning.
MATERIALS AND METHODS
This is a retrospective analysis of data available in our system from January 2017 to June 2020. All the patients with the diagnosis of intracranial meningiomas were included in the study. A total of 21 patients were included in the study. No ethical clearance was required as this is a retrospective analysis not affecting the patient outcome.
All patients underwent magnetic resonance imaging (MRI) on a 1.5Tesla MR scanner (Siemen’s Symphony, Erlangen, Germany). The sequences used were as per [Table 1] (SE T1, TSE T2, fluid-attenuated inversion recovery and gradient echo axial, TSE T2 coronal, and T1 3D sag. Post-contrast images were also obtained in all three planes). DWI was carried out at b values of 0, 500, and 1000 s/mm2. The images were analyzed at the workstation. DW images were visually inspected and classified as hyperintense, isointense, or hypointense compared with normal white matter. The apparent diffusion coefficient (ADC) images were autogenerated. The ADC value of lesions (meningiomas) was calculated using at least 1 Sq Cm region of interest (ROI). Lesions less than 1 cm in size were excluded from the study. ADC values were recorded from the ADC maps for a solid portion of the tumor, for the contralateral normal area, and for edema (these regions were sampled, avoiding the cystic and necrotic areas), by drawing the circular ROI manually, on all axial ADC maps, using the manufacturer’s software. For the tumor-giving variable SI, the highest intensity ROI was selected and its SI was noted. In some cases, more than 1 ROI was drawn and an average ADC value was recorded. ADC of the tumor was divided by the ADC of the normal white matter to find the normalized ADC (NADC) ratios, considering NADCs <1.00 represent relatively restricted diffusion. [Figures 1 and 2] show the representative MRI images of Grade I and Grade II meningiomas, respectively.
| S. No. | Sequences | TR | TE | FOV | Concatenation |
|---|---|---|---|---|---|
| 1. | T1WI | 560 msec | 7.7 msec | 230 mm | 1 |
| 2. | T2WI | 5300 msec | 110 msec | 230 mm | 1 |
| 3. | Fluid-attenuated inversion recovery | 8600 msec | 88 msec | 230 mm | 2 |
| 4. | Gradient echo | 870 msec | 26 msec | 250 mm | 1 |
| 5. | Diffusion-weighted with apparent diffusion coefficient map | 4200 msec | 94 msec | 250 mm | 1 |
| 6. | T2W coronal | 5400 msec | 120 msec | 230 mm | 1 |
| 7. | Flash 3d T1 MP rage sag | 11 msec | 5.2 msec | 250 mm | 1 |
| 8. | Pre-and post-contrast T1FS axial | 530 msec | 9.4 msec | 230 mm | 2 |
MRI: Magnetic Resonance Imaging, T1WI - T1 weighted imaging, T2WI - T2 weighted imaging, T1FS - T1 Fat suppressed

- (a-c) A large meningioma in the left frontoparietal region showing restriction on DWI. This was a Grade 1 meningioma.

- (a-e) A large left parafalcine meningioma in the frontal region showing no significant restriction of diffusion on DWI. This was a Grade 2 meningioma.
We used ADC value as a primary parameter to type the menigioma as typical or atypical. We also considered atypical morphological features as a secondary parameter. Further, the findings were correlated with histopathological reports of grading of meningioma.
For statistical analysis, the MedCalc software package was used (MedCalc Statistical Software version 14.8.1, MedCalc Software bvba, Ostend, Belgium). Collected data were evaluated using descriptive statistics. Spearman’s correlation coefficient was used to analyze the association between ADC/NADC values and histological parameters. P < 0.05 was taken to indicate statistical significance in all instances. The receiver operating characteristic curve analysis was not performed due to the paucity of Grade II lesions.
RESULTS
There were 21 cases enrolled in this study (from January 2017 to June 2020) who underwent imaging as well as surgery. Their findings are tabulated in [Table 2]. In our study, there were 13 males and eight females. The age range was 14–77 years with a mean age of 52 years. Out of the total of 21 cases, 20 cases (95.2%) were of WHO Gr 1 while 1 case (4.8%) was of WHO Gr 2 on histopathological examination (HPE). There were 10 cases of transitional meningioma, 5 cases of meningothelial meningioma, three cases of angiomatous meningioma, and one case each of fibroblastic and psammomatous meningioma and a solitary case of clear cell meningioma (WHO Grade II).
| S. No. | Age | Sex | Normalized ADC value (10−3s/mm2) | HPE |
|---|---|---|---|---|
| 1. | 14 years | M | 0.178 | Angiomatous and microcystic meningioma (WHO Grade 1) |
| 2. | 62 years | M | 0.91 | Meningothelial meningioma (WHO Grade 1) |
| 3. | 37 years | M | 0.90 | Meningothelial meningioma (WHO Grade 1) |
| 4. | 46 years | F | 1.375 | Fibroblastic meningioma (WHO Grade 1) |
| 5. | 38 years | M | 1.35 | Transitional meningioma (WHO Grade 1) |
| 6. | 41 years | M | 1.22 | Angiomatous variant, (WHO Grade 1) |
| 7. | 40 years | M | 1.04 | Meningothelial meningioma (WHO Grade 1) |
| 8. | 54 years | M | 1.05 | Transitional meningioma, (WHO Grade 1) |
| 9. | 70 years | F | 1.10 | Psammomatous meningioma (WHO Grade 1) |
| 10 | 50 years | M | 1.09 | Meningothelial meningioma (WHO Grade 1) |
| 11. | 48 years | F | 1.26 | Clear cell meningioma (WHO Grade 2) |
| 12. | 77 years | F | 1.10 | Transitional meningioma (WHO Grade 1) |
| 13. | 63 years | M | 1.06 | Transitional meningioma (WHO Grade 1) |
| 14. | 67 years | F | 1.04 | Transitional meningioma (WHO Grade 1) |
| 15. | 40 years | F | 1.18 | Transitional meningioma (WHO Grade 1) |
| 16. | 60 years | F | 1.17 | Transitional meningioma (WHO Grade 1) |
| 17. | 67 years | F | 1.04 | Meningothelial meningioma (WHO Grade 1) |
| 18. | 19 years | M | 1.10 | Angiomatous meningioma (WHO Grade 1) |
| 19. | 73 years | M | 0.247 | Transitional meningioma (WHO Grade 1) |
| 20. | 70 years | M | 0.88 | Transitional meningioma (WHO Grade 1) |
| 21. | 58 years | M | 0.14 | Transitional meningioma (WHO Grade 1) |
ADC: Apparent Diffusion Coefficient, HPE: Histopathological Examination, M: Male, F - Female
The analysis of NADC values in the group of Grade I meningioma showed that in 6 cases (28%), the value was <1, while in 14 cases (66%), it was more than 1. In the solitary case of Gr 2 meningioma in our series, the NADC was higher than 1. There was no significant correlation between the NADC values and WHO grading of the tumor (r = 0.18, P = 0.41) in our series of cases. However, we observed a weak correlation between the NADC values and various histological subtypes of meningiomas (r = 0.35, P = 0.11) which was not significant. A scatter plot is shown in [Figure 3] to illustrate the same.
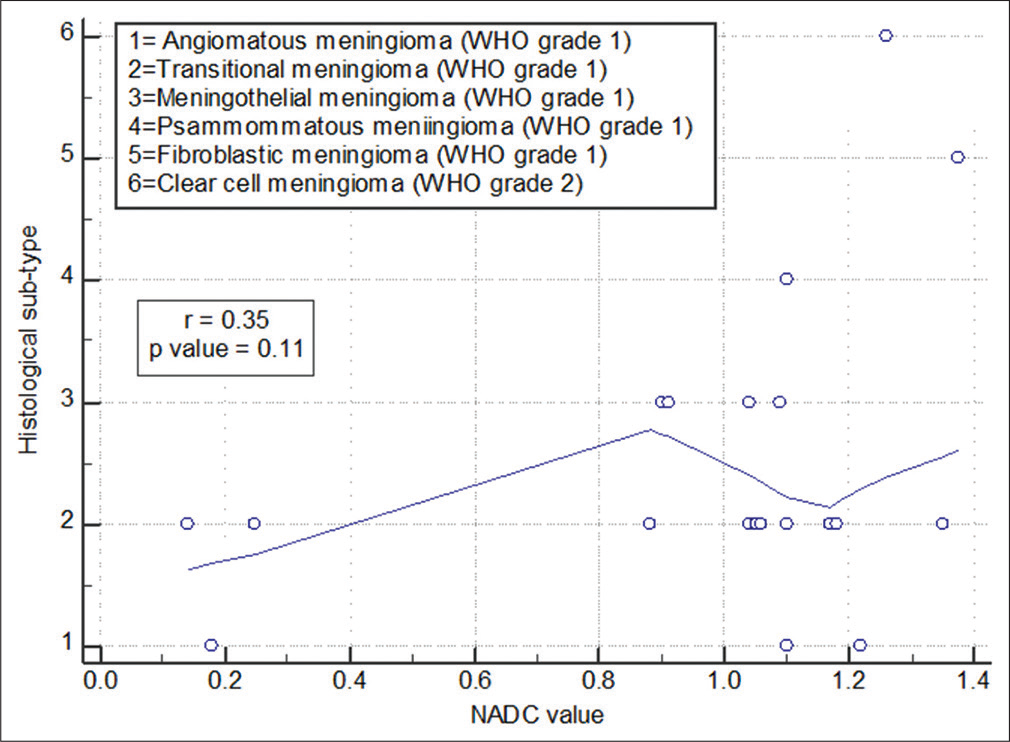
- Scatter plot showing correlation between the NADC values and histological subtypes of meningioma.
DISCUSSION
There have been mixed reports of reports on the role of ADC value in deciding the grades of meningioma vis-avis histopathology. Pre-operative diagnosis of high-grade meningiomas will alter the management. Higher grades of meningioma may require radiotherapy besides surgery.[5] However, some workers have predicted a strong correlation between the grades of the tumor on HPE vis-a-vis ADC values. Hakyemez et al. found that the mean ADC value of benign tumors was significantly more than the ADC value of atypical/malignant meningiomas, namely, 1.17 ± 0.21 × 10−3 mm2s−1 and 0.75 ± 0.21 × 10−3 mm2s−1, respectively (P < 0.001).[6]
Abdel-Kerim et al. in their series of 70 meningiomas in 68 patients found a higher ADC value in Gr II meningiomas but not in Gr I meningiomas. In their series, the authors concluded that 0.79 × 10−3 mm2/s is the cutoff value for deciding the restriction on DWI.[7] Comparative values by Nagar et al. (0.89 × 10−3 mm2/s) and Tang et al. (0.70 × 10−3 mm2/s) have proposed for restriction on DWI.[8,9] Atypical meningiomas, exhibit small cells with high mitotic activity, increased nuclear-to-cytoplasmic ratio, uninterrupted growth pattern, large nucleoli, and necrosis.[10] The role of the intracellular environment in the restriction of diffusion is not entirely clear. Diffusion is restricted by membranes, tight cell junctions, fibers, and probably to a lesser degree, macromolecules and nuclear-to-cytoplasmic ratio.[11,12] High-grade brain tumors with increased cellularity have lower ADC values. Cellularity is considered to be the main factor affecting the diffusion of water molecules in living tissue.[13]
In our study, there is no significant correlation between the grades of meningioma versus the ADC value. The NADC values varied from 0.14 to 1.37 × 10−3 mm2/s for Gr I meningioma in our series though most of our cases fell in this category of meningioma. Although we had a solitary case of Gr-II meningioma, the ADC value exhibited was 1.26 × 10−3 mm2/s.
The ADC values can be variable on the acquisition and can be machine specific. We have used NADC in our study to obviate these factors.
Pavlisa et al. found the ADC value in typical meningiomas to be 0.939 versus 0.917 in atypical meningiomas and deciphered that ADC value is not helpful in pre-operative grading of the meningioma. We, in our studies, have a higher NADC value as compared to Pavlisa et al. to reach a similar conclusion.[14]
Our study is unique in the sense that we have utilized NADC vis-a-vis ADC value to minimize the machine-specific variability. The shortcoming of our study is the small sample size with a low number of higher-grade meningiomas.
However, a review of the literature reveals a mixed bag of results for using ADC value. In addition, even fewer studies have used NADC value to characterize meningiomas.
CONCLUSION
Meningiomas are a common group of tumors in the brain with a quest to characterize the grades preoperatively on imaging. The NADC is a better method as compared to plain ADC values. In our series, we did not find any correlation of NADC on pre-operative imaging to the grades of tumors.
Author’s contribution
Samaresh Sahu conceptualised the design of this study. Saurabh Maheshwari and Saikat Bhattacharjee contributed to the acquisition and analysis of patient data and images.
Vibhuti Maria and Pushkar Mendiratta contributed to the drafting and revision of the manuscript.
Rakesh Kumar contributed to the interpretation of images.
All authors have agreed both to be personally accountable for their own contributions and they have ensured that questions related to the accuracy or integrity of any part of this work, even ones in which they were not personally involved, were appropriately investigated, resolved, and the resolution was documented in the literature.
All authors have read and approved the manuscript.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Meningioma grading: An analysis of histologic parameters. Am J Surg Pathol. 1997;21:1455-65.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of atypical and anaplastic meningiomas: A review. Neurosurgery. 2005;57:538-50.
- [CrossRef] [PubMed] [Google Scholar]
- Grading astrocytic tumors by using apparent diffusion coefficient parameters: Superiority of a one-versus two-parameter pilot method. Radiology. 2009;251:838-45.
- [CrossRef] [PubMed] [Google Scholar]
- Is diffusion-weighted imaging useful in grading and differentiating histopathological subtypes of meningiomas? Eur J Radiol. 2012;81:2389-95.
- [CrossRef] [PubMed] [Google Scholar]
- Grade 2 meningioma and radiosurgery. J Neurosurg. 2015;122:1157-62.
- [CrossRef] [PubMed] [Google Scholar]
- The contribution of diffusion-weighted MR imaging to distinguishing typical from atypical meningiomas. Neuroradiology. 2006;48:513-20.
- [CrossRef] [PubMed] [Google Scholar]
- Differentiation between benign and atypical cranial Meningiomas. Can ADC measurement help? MRI findings with histopathological correlation. Egypt J Radiol Nucl Med. 2018;49:172-5.
- [CrossRef] [Google Scholar]
- Diffusion-weighted MR imaging: diagnosing atypical or malignant meningiomas and detecting tumor dedifferentiation. Am J Neuroradiol. 2008;29:1147-52.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of apparent diffusion coefficient with Ki67 proliferation index in grading meningioma. Am J Roentgenol. 2014;202:1303-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pathology and Genetics of Tumours of the Nervous System Geneva: World Health Organization Classification of Tumours; 2000. p. :176-89.
- [Google Scholar]
- Diffusion theory in biology: A relic of mechanistic materialism. J Hist Biol. 2000;33:71-111.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanism of detection of acute cerebral ischemia in rats by diffusion-weighted magnetic resonance microscopy. Stroke. 1992;23:746-54.
- [CrossRef] [PubMed] [Google Scholar]
- Inverse correlation between choline magnetic resonance spectroscopy signal intensity and the apparent diffusion coefficient in human glioma. Magn Reson Med. 1999;41:2-7.
- [CrossRef] [Google Scholar]
- Characteristics of typical and atypical meningiomas on ADC maps with respect to schwannomas. Clin Imaging. 2008;32:22-7.
- [CrossRef] [PubMed] [Google Scholar]




